Back to Journals » Infection and Drug Resistance » Volume 18
Diabetes Mellitus and the Risk and Outcomes of Clostridioides Difficile Infection: A Systematic Review
Authors Zhang Q, Zhou M, Shi L, Fang Z
Received 22 August 2025
Accepted for publication 27 October 2025
Published 4 November 2025 Volume 2025:18 Pages 5685—5701
DOI https://doi.org/10.2147/IDR.S562597
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hazrat Bilal
Qiongfang Zhang,1 Min Zhou,2 Lili Shi,3 Ze Fang2
1Department of Hospital Infection Management, Zhongjiang County People’s Hospital, Deyang, Sichuan, People’s Republic of China; 2Department of Endocrinology, Zhongjiang County People’s Hospital, Deyang, Sichuan, People’s Republic of China; 3Department of Geriatrics, Zhongjiang County People’s Hospital, Deyang, Sichuan, People’s Republic of China
Correspondence: Ze Fang, Email [email protected]
Background: Patients with diabetes mellitus (DM) are at increased risk for Clostridioides difficile (C. difficile) infection (CDI), in part due to frequent exposure to antibiotics—particularly broad-spectrum agents—which represents the most important modifiable risk factor for CDI.
Objective: To systematically evaluate the impact of DM on the incidence and recurrence risk of CDI, explore underlying mechanisms, and provide evidence-based guidance for prevention and control in high-risk populations.
Methods: A systematic search was conducted in PubMed, Embase, and Web of Science to identify cohort and case-control studies reporting on the association between diabetes and the risk or outcomes of CDI. The ROBINS-I tool was used for risk of bias assessment. Random-effects models were applied to pool odds ratios (ORs) and 95% confidence intervals (CIs). Subgroup analyses, sensitivity analyses, and cumulative meta-analyses were performed. The quality of evidence for the primary outcomes was graded according to the GRADE approach. The study protocol was registered in PROSPERO (registration number: CRD420251128182).
Results: A total of 12 international studies (including 8 reporting recurrence outcomes) and covering more than 3. 5 million participants from North America, Europe, and East Asia were included. Meta-analysis showed that diabetes significantly increased the risk of CDI (OR=1. 46, 95% CI: 1. 20– 1. 77), as well as the risk of recurrence (OR=3. 11, 95% CI: 1. 98– 4. 87). Subgroup and sensitivity analyses yielded consistent results, and cumulative meta-analysis indicated that effect sizes became stable over time. Mechanistic analyses suggested that immune dysfunction, gut microbiota imbalance, and exposure to high-risk medications were key contributing factors. Based on GRADE assessment, the quality of evidence for the primary outcomes was moderate, with a low risk of publication bias.
Conclusion: Diabetes is an independent risk factor for both CDI and its recurrence. It is recommended that clinicians strengthen CDI risk assessment and integrated prevention strategies for patients with diabetes, with a focus on optimizing antibiotic stewardship, reducing unnecessary broad-spectrum antibiotic use, and microbiota-targeted interventions. High-quality prospective studies are needed to further improve prevention strategies and elucidate underlying mechanisms.
Plain Language Summary: This is the first meta-analysis to assess both the risk of developing and recurring C. difficile infection (CDI) in people with diabetes.
Diabetes increases CDI risk due to immune system problems, gut microbiota changes, and chronic inflammation.
We carefully considered antibiotic and proton pump inhibitor (PPI) use, making our results more reliable.
The findings support better infection control and prevention strategies for diabetic patients.
Special attention is needed in China and East Asia, where antibiotic use and gut microbiota patterns differ from Western countries.
Keywords: diabetes mellitus, Clostridioides difficile infection, recurrence, infection risk, mechanism, clinical outcomes
Introduction
Background
Clostridioides difficile (C. difficile) is a leading cause of hospital-acquired diarrhea worldwide. The incidence and mortality of Clostridioides difficile infection (CDI) have risen significantly in recent years, posing a serious public health challenge.1 In the United States, CDI accounted for an estimated 453,000 infections and nearly 29,300 deaths in 2011.2 Molecular epidemiological studies from China also report a growing prevalence of CDI and the emergence of hypervirulent strains in hospital settings.3 Only toxigenic C. difficile strains are clinically relevant, as their pathogenicity depends on the production of toxins A (TcdA) and B (TcdB); some strains also produce a binary toxin, which may increase disease severity. Hypervirulent strains, such as ribotype 027, are associated with more severe and recurrent infections.4 CDI not only increases in-hospital mortality and healthcare burden, but is also associated with prolonged hospital stays and higher medical costs.5 With the ongoing aging of the population and increasing prevalence of chronic diseases, the demographic structure of populations susceptible to CDI and at risk for poor outcomes is changing.
Diabetes mellitus (DM) is a globally prevalent metabolic disorder with a rising incidence.1,5 Due to impaired immune function and alterations in gut microbiota, patients with diabetes are more susceptible to infections, especially intestinal infections such as CDI.6 Several large retrospective studies have found that the risk of CDI is significantly higher in patients with diabetes than in those without, and this risk has been increasing over time.1,5,7 In hospitalized patients, diabetes is not only an independent risk factor for CDI, but is also associated with higher risks of recurrence, severe disease, and mortality.5,8 Patients with CDI and comorbid diabetes often have additional underlying conditions, such as heart failure, renal insufficiency, or malignancies, further exacerbating the disease burden and risk of poor outcomes.7
Besides underlying diseases, widespread use of antibiotics and acid-suppressive agents is another important risk factor for CDI.9,10 Because of recurrent infections and complication treatments, diabetic patients are more frequently exposed to broad-spectrum antibiotics and proton pump inhibitors (PPIs), increasing both their susceptibility to and complexity of CDI.3,9,10
Such increased antibiotic and PPI exposure is recognized as a primary driver of CDI risk, as these agents disrupt the gut microbiota and diminish colonization resistance to C. difficile.6,9,10
The epidemiology of CDI varies across geographic regions and healthcare settings. In environments such as nursing homes and long-term care facilities, the incidence of CDI among diabetic patients is higher than in the general population, and infections are more likely to be recurrent and persistent.7,11 In patients with other underlying diseases, such as inflammatory bowel disease (IBD), the coexistence of diabetes further increases the incidence and mortality of CDI and related complications, reflecting a synergistic adverse effect.6
Immune dysfunction, gut microbiota imbalance, and frequent exposure to high-risk medications—especially broad-spectrum antibiotics (eg, clindamycin, cephalosporins, fluoroquinolones) and proton pump inhibitors (PPIs)—make diabetic patients a high-risk group for CDI.6,9,10 The combination of these factors leads to a substantially higher CDI risk in diabetic compared to non-diabetic populations.
CDI in diabetic patients not only significantly increases disease burden, hospitalization, and mortality, but also imposes greater pressure on healthcare resources. Therefore, early identification, precise prevention, and individualized treatment of CDI in patients with diabetes are crucial for reducing recurrence and improving outcomes.1,5–7
Although international studies have shown that diabetes significantly increases the risk of CDI, systematic comparisons across different ethnic groups, healthcare systems, and medication use backgrounds remain limited. Notably, Asian countries and Western developed nations differ markedly in antibiotic stewardship, gut microbiota composition, and the spectrum of underlying diseases.
China is among the world’s largest consumers of antibiotics; recent national surveillance reported antibiotic consumption reaching 13.9 defined daily doses (DDD) per 1000 inhabitants per day in 2019, substantially higher than most high-income Western countries.12 Both community and hospital antibiotic management face major challenges, and the proportion of high-risk medications such as broad-spectrum antibiotics and proton pump inhibitors (PPIs) is also considerably higher than in Western countries. These factors may lead to distinct epidemiological characteristics regarding CDI susceptibility and recurrence among Chinese diabetic patients.
Additionally, East Asian populations differ from Western populations in the age of diabetes onset, complication profiles, and gut microbiota structure. Therefore, there is an urgent need for large, multicenter systematic reviews and meta-analyses to clarify the risk and outcomes of CDI among diabetic patients in China and East Asia and to provide evidence-based guidance for local prevention and control strategies.However, high-quality systematic reviews and meta-analyses on the association between diabetes and CDI risk in China are still scarce, and the underlying mechanisms and effective interventions remain inadequately defined,1,5,8–11,13 highlighting a critical evidence gap in this field.
Thus, systematically evaluating the impact of diabetes on the occurrence and prognosis of CDI is of great significance for the precise identification of high-risk populations, optimization of prevention and control strategies, and improvement of clinical outcomes.
Research Questions and Objectives
Previous studies suggest that diabetes mellitus may increase the risk of C. difficile infection (CDI) through multiple mechanisms and may adversely affect clinical outcomes following infection.However, there is still insufficient systematic evidence regarding the association between diabetes and CDI, particularly with respect to the impact on different outcomes such as the risk of initial CDI, recurrence rates, severity, and mortality. This study aims to systematically evaluate, through a systematic review and meta-analysis, the effects of diabetes on the risk of CDI and adverse outcomes, and to investigate the modifying effects of key related covariates on this association. The specific research questions include:
- Does diabetes mellitus increase the risk of incident CDI (initial occurrence) among hospitalized or community-dwelling adults?
- Among patients with confirmed CDI, does diabetes mellitus increase the risk of adverse outcomes such as recurrence, severity, or mortality?
Methods
Study Design and Registration
This study was conducted as a systematic review and meta-analysis, designed and reported in strict accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines.14 The study protocol was registered in the international PROSPERO database to ensure transparency and reproducibility (registration number: CRD420251128182). This meta-analysis was carried out around pre-specified research questions, involving systematic literature search, screening, and inclusion based on unified criteria for data extraction and quality assessment.The association between diabetes mellitus and the risk and clinical outcomes of C. difficile infection was quantitatively synthesized and evaluated.
Literature Search Strategy
A systematic search was conducted in three major databases—PubMed, Embase, and Web of Science—from their inception until August 2025, aiming to identify all studies related to the risk and outcomes of C. difficile infection in patients with diabetes mellitus. The search strategy incorporated both MeSH terms and free-text keywords, with the main search topics including “diabetes mellitus”, “Clostridium difficile infection”, “risk”, and “outcome”. The complete English search strategies and the results for each database are detailed in Supplementary Table S1.
Inclusion and Exclusion Criteria
Inclusion Criteria:
- The study population comprised adults (≥18 years) from either inpatient or community settings;
- Studies explicitly reported the association between diabetes mellitus and C. difficile infection (CDI), with a clear distinction between diabetic and non-diabetic status;
- Effect estimates (such as OR, RR, HR, and their 95% confidence intervals) or raw frequency data could be extracted;
- Cohort studies, case-control studies, or comparable cross-sectional studies were included;
- Full-text articles were available.
Exclusion Criteria:
- Studies exclusively involving pediatric populations;
- Studies without a control group or those unable to distinguish between diabetic and non-diabetic status;
- Studies available only as abstracts without data, or full texts could not be obtained;
- Animal experiments, in vitro studies, editorials, reviews, case series, or case reports;
- Duplicate publications—only the most comprehensive report was included.
Data Extraction and Management
Four investigators independently screened the literature and extracted data according to unified standards. The extracted data included: first author, year of publication, country or region, study design, total sample size, sample size in the diabetes group, sample size in the non-diabetes group, mean age, percentage of female participants, CDI susceptibility among diabetic patients, CDI recurrence among diabetic patients, and whether key covariates such as antibiotic and PPI use were adjusted for.All extracted data were recorded in standardized tables, and any discrepancies were resolved through team discussion until consensus was reached. In cases where key information was missing, attempts were made to contact the original authors to ensure data completeness and accuracy.
Risk of Bias Assessment
The ROBINS-I (Risk Of Bias In Non-randomized Studies - of Interventions) tool was used to assess the risk of bias in all included non-randomized studies.15 ROBINS-I is an internationally recognized tool for evaluating the risk of bias in non-randomized studies, covering seven domains: confounding, selection, classification of exposures, intervention measurement, missing data, outcome measurement, and reporting bias. Four investigators independently assessed each study in all domains. Any disagreements were first resolved through team discussion; if consensus could not be reached, a third senior investigator was consulted for final adjudication. Detailed judgments for each domain of every study are documented in Supplementary Table S2 to ensure the transparency and traceability of the evaluation.
Outcome Definitions and Statistical Analysis
Outcome A: CDI susceptibility in diabetes refers to the risk of developing C. difficile infection (CDI) among patients with diabetes, measured by comparing the incidence of CDI between diabetic and non-diabetic populations. The results are presented as odds ratios (ORs) with 95% confidence intervals (CIs).
Outcome B: CDI recurrence in diabetes refers to the risk of recurrent CDI among patients with diabetes after an initial episode. The recurrence rates between the diabetes and non-diabetes groups are compared, and the results are expressed as ORs with 95% CIs.
Statistical Analysis
Meta-analyses were conducted using R software.Pooled effect estimates were calculated using either random-effects or fixed-effect models, depending on the heterogeneity (assessed by the I2 statistic and Cochran’s Q test). Heterogeneity was evaluated with the I2 and Q statistics, and pooled ORs with 95% CIs were reported, along with forest plots.Sensitivity analyses and subgroup analyses were performed as needed to explore sources of heterogeneity and the robustness of the results. Publication bias was assessed using funnel plots and the Egger’s test. All statistical tests were two-sided, and a p-value of <0.05 was considered statistically significant.
Subgroup and Sensitivity Analyses
Subgroup analyses were conducted based on the following variables: study design, sample size, and mean age.These analyses aimed to explore the impact of different study characteristics on the pooled effect estimates and to assess the stability of the results.Sensitivity analyses were performed by sequentially excluding individual studies and by including only high-quality studies, in order to evaluate the robustness of the primary findings and to assess the potential influence of studies at high risk of bias on the overall conclusions. All analyses were performed using R software to ensure scientific rigor and reliability.
Evidence Grading (GRADE)
The quality of evidence for the primary outcomes in this study was assessed using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach.The GRADE system systematically evaluates each primary outcome across five domains: risk of bias, imprecision, inconsistency, indirectness, and publication bias.The quality of evidence is then rated as high, moderate, low, or very low (Supplementary Table S3).
Results
Literature Screening Process
A total of 910 articles were initially identified in the literature search. After removing duplicates, 630 unique articles remained. Following title and abstract screening, 547 articles were excluded, leaving 83 articles for full-text assessment.Of these, 13 articles were excluded due to inaccessible full text.The main reasons for excluding other articles during full-text review included: study population not meeting inclusion criteria or being pediatric, exposure or outcomes not relevant to the research topic, data not extractable, or non-human studies.Ultimately, 12 studies were included in the meta-analysis. The detailed screening process and reasons for exclusion are shown in the PRISMA flow diagram (Figure 1).
 |
Figure 1 PRISMA Flow Diagram of Study Selection. |
Main Characteristics of Included Studies
A total of 12 studies were included in this meta-analysis, spanning several countries including the United States, Spain, the United Kingdom, Poland, Canada, South Korea, and Costa Rica.The study designs comprised retrospective cohort studies and case-control studies. The total sample size of the included studies ranged from 143 to 3,491,000 participants, with sample sizes for the diabetes and non-diabetes groups reported separately. The mean age of study populations ranged from 57.65 to 81.10 years, and the proportion of female participants ranged from 32.0% to 69.7%.All studies reported effect estimates for the association between diabetes and susceptibility to C. difficile infection, with some studies additionally reporting on CDI recurrence risk.Some studies adjusted for covariates such as antibiotic and PPI use.All studies were assessed as having a moderate risk of bias using the ROBINS-I tool.The main characteristics of the included studies are summarized in Table 1.
 |
Table 1 Main Characteristics of Included Studies |
Risk of CDI Susceptibility and Recurrence in Diabetes Mellitus
This meta-analysis included 12 studies to comprehensively evaluate the risks associated with diabetes mellitus and C. difficile infection (CDI). The pooled results showed that patients with diabetes had a significantly higher risk of developing CDI compared to non-diabetic individuals, with a pooled OR of 1.46 (95% CI: 1.20–1.77, P=0.0012), and moderate heterogeneity among studies (I2=50.5%; see Figure 2).For the risk of CDI recurrence, 8 relevant studies were included, and the pooled OR was 3.11 (95% CI: 1.98–4.87, P=0.0006), with a higher degree of heterogeneity (I2=69.3%; see Figure 3).
 |
Figure 2 Forest Plot of Meta-analysis for the Risk of CDI in Patients with Diabetes Mellitus. |
 |
Figure 3 Forest Plot of Meta-analysis for the Risk of CDI Recurrence in Patients with Diabetes Mellitus. |
Publication bias was assessed using funnel plots for both CDI susceptibility and recurrence risk (Figure 4), with no obvious small-study effects observed. Begg’s test did not reveal significant publication bias for CDI susceptibility (z = −0.14, P = 0.8909), while Egger’s test was positive (t = 2.50, P = 0.0316), suggesting possible small-study bias for this outcome. The funnel plots appeared generally symmetrical, and considering both statistical tests and the number of included studies, the overall risk of publication bias was low, but these conclusions should still be interpreted with caution. Current evidence demonstrates that patients with diabetes have significantly higher risks for both initial CDI and recurrence compared to non-diabetic individuals. The results of this study are robust; however, given the moderate to high heterogeneity in some analyses and the potential small-study effects indicated by publication bias tests, further high-quality, large-sample studies are warranted to validate these conclusions.
 |
Figure 4 Funnel Plots for Publication Bias in Meta-analyses of CDI Risk and Recurrence in Diabetes Mellitus. |
Subgroup and Sensitivity Analyses
To comprehensively assess the sources of heterogeneity and the robustness of the main findings, this study performed subgroup analyses on core characteristics affecting effect estimates, and applied the leave-one-out method for sensitivity analysis.
In the subgroup analyses, regardless of stratification by study design, sample size, or mean age, diabetes mellitus consistently and significantly increased the risk of CDI, with the direction of the pooled effect sizes remaining stable across all subgroups. Specifically, both retrospective cohort studies and case-control studies yielded a pooled OR of 1.47, but the heterogeneity was significantly higher in cohort studies (I2 = 61.6%) than in case-control studies (I2 = 0%), suggesting that large database studies may have differences in population structure, data collection methods, or follow-up strategies, contributing to fluctuations in effect size. The number and types of covariates adjusted for in some cohort studies also varied, further increasing uncertainty. Heterogeneity in the large-sample group (I2 = 65.7%) was much higher than in the small-sample group (I2 = 4.9%), which may be attributed to the fact that large-sample cohorts are often multicenter or database-based, with greater variability in patient types and data collection methods.In contrast, small-sample studies are usually single-center with higher methodological consistency, resulting in lower heterogeneity. The inclusion of incomplete subgroup data or complex population structures in large-sample studies may introduce confounding factors and further exacerbate heterogeneity.
When stratified by mean age in the susceptibility analysis, the heterogeneity was moderate in the >65-year-old group (I2 = 52.7%) and very low in the <65-year-old group (I2 = 5.1%), suggesting that differences in comorbidities, treatment approaches, and diagnostic criteria among elderly patients are important sources of heterogeneity.In the recurrence risk analysis, however, higher heterogeneity was observed in the <65-year-old group (I2 = 83.9%) compared to the >65-year-old group (I2 = 53.2%).This indicates that methodological and statistical heterogeneity may be more pronounced in younger patient subgroups regarding recurrence risk.The limited number of studies in some subgroups also resulted in wide confidence intervals, underscoring the need for larger samples and more regionally diverse data for further validation (see Table 2 and Supplementary Figure S1).
 |
Table 2 Summary Table of Subgroup Analyses and Heterogeneity |
For the analysis of sources of heterogeneity, to further explore the heterogeneity in recurrence risk, meta-regression analyses were performed using publication year, mean age, and sample size as study-level covariates.The results showed that none of these covariates could significantly account for the observed heterogeneity in this outcome, as the R2 values of the meta-regression models were close to zero or not statistically significant, and the residual heterogeneity (I2) remained high. This suggests that conventional study characteristics reported in the current literature are insufficient to explain the effect size differences for this outcome, and that the observed heterogeneity may arise from unreported clinical or methodological factors, such as comorbidities, variations in interventions, or inconsistent diagnostic criteria. Future studies are therefore recommended to improve the standardized reporting of key covariates to facilitate subsequent evidence-based analyses.
Sensitivity analysis was performed using the leave-one-out approach to assess the influence of individual studies on the overall effect estimates. The results showed that, for both CDI susceptibility and recurrence risk, sequential exclusion of each study did not result in substantial changes in the pooled effect sizes, and the confidence intervals remained highly overlapping, further supporting the robustness of the main conclusions (Figure 5).
 |
Figure 5 Sensitivity Analysis Plot. |
Cumulative meta-analysis demonstrated that, as the number of included studies increased, the pooled effect sizes for diabetes and both CDI susceptibility and recurrence risk gradually stabilized, with confidence intervals narrowing significantly. This indicates that the overall analysis results are robust, and that recently published studies have not materially affected the main conclusions (Figure 6).
 |
Figure 6 Cumulative Meta-analysis Plot. |
In summary, the current meta-analysis findings demonstrate good consistency across different study designs, sample sizes, and age structures, and are not dominated by any single study, suggesting scientific reliability. However, it should be noted that heterogeneity remains notable in large-sample studies, cohort designs, and elderly populations, reflecting the complexity and diversity of real-world clinical research.
GRADE Evidence Quality Assessment
The quality of evidence for the two primary outcomes was evaluated using the GRADE approach. The results showed that the quality of evidence regarding the association between diabetes mellitus and the risk of C. difficile infection was moderate, while the quality of evidence for CDI recurrence risk was low to moderate.The main reasons for downgrading included the observational nature of all included studies (risk of bias), moderate to high heterogeneity (inconsistency), and potential publication bias for the CDI susceptibility outcome. No domains warranted upgrading.A detailed evaluation for each outcome is provided in Supplementary Table S3. Overall, the existing evidence is relatively reliable, but further high-quality, prospective studies are needed for additional validation.
Discussion
Summary of Main Findings
This meta-analysis systematically evaluated the association between diabetes mellitus and both the risk and recurrence of C. difficile infection (CDI). Pooled results from 12 studies showed that patients with diabetes have a significantly higher risk of both CDI and its recurrence compared to non-diabetic individuals. Subgroup and sensitivity analyses confirmed the robustness of the main findings. Overall, diabetes mellitus is an important independent risk factor for both CDI and its recurrence.
Mechanistic Insights and Clinical Implications
Effects of Diabetes on Host Immunity, Gut Microbiota, and Inflammatory Responses
Diabetes predisposes patients to both initial and recurrent C. difficile infection (CDI) through several interconnected mechanisms, as supported by our meta-analysis and previous studies.
Chronic hyperglycemia impairs both innate and adaptive immune responses.Reduced neutrophil and macrophage function, along with lower antibody production, weakens host defense against C. difficile and its toxins.1,5,16 This immunosuppression is reflected in large-scale cohort studies showing a persistently higher CDI risk among people with diabetes.
Diabetes leads to gut microbiota dysbiosis—characterized by decreased beneficial bacteria (eg, Bifidobacterium, Lactobacillus) and increased colonization by pathogens including C. difficile.Use of antibiotics—particularly clindamycin, cephalosporins, and fluoroquinolones—and proton pump inhibitors (PPIs), which are more frequent in diabetic patients, further disrupts microbial balance and diminishes resistance to CDI.17–19 This dysbiosis also compromises the intestinal barrier and immune homeostasis.
Heightened inflammatory responses are common in diabetes. Hyperglycemia activates systemic and gut inflammatory pathways (such as TLRs and the NLRP3 inflammasome), increasing pro-inflammatory cytokine release (eg, IL-1β, TNF-α) and intestinal permeability, which facilitates pathogen and toxin invasion.5,18
The interaction of immune dysfunction, microbiota imbalance, and inflammation contributes to the higher risk and recurrence of CDI observed in diabetic patients in our study. These mechanisms highlight the need for early risk assessment and tailored prevention strategies in this vulnerable population5,16–18.
Why Are CDI Susceptibility and Recurrence Risks Elevated in Diabetic Populations?
The significantly increased susceptibility and recurrence risk of CDI among patients with diabetes result from the combined effects of multiple factors. Chronic exposure to hyperglycemia in diabetes leads to persistent impairment of the immune barrier, reducing the body’s ability to defend against pathogens, especially those causing intestinal infections. Recent research demonstrates that hyperglycemia impairs innate immunity by disrupting neutrophil and macrophage function, weakening the mucosal barrier, and promoting a chronic pro-inflammatory state. These changes together increase both the susceptibility to, and severity of, bacterial infections, including CDI.20 Studies have shown that the incidence of CDI and rates of rehospitalization are markedly higher in diabetic populations than in non-diabetic patients, and that diabetes itself is an important independent predictor of CDI recurrence and mortality.1,5,16
Due to the complexity of their underlying diseases, diabetic patients are often hospitalized more frequently and have significantly higher rates of exposure to high-risk medications, especially broad-spectrum antibiotics such as clindamycin, cephalosporins, and fluoroquinolones, as well as proton pump inhibitors (PPIs), all of which have been proven to strongly promote the occurrence and recurrence of CDI. Relevant literature reports that, during antibiotic treatment, diabetic individuals are more likely to experience gut microbiota imbalance, with reductions in probiotics and increased colonization of C. difficile, resulting in weakened microbial defenses.18,19 Further evidence from studies in high-risk populations such as those with inflammatory bowel disease has confirmed that patients with concomitant diabetes have significantly higher risks of CDI, recurrence, and related adverse outcomes than those with a single underlying disease, indicating that the combination of metabolic disorders and immune dysfunction synergistically amplifies the clinical impact of CDI.17
The chronic inflammatory state and impaired intestinal barrier function associated with diabetes further exacerbate susceptibility to CDI and the tendency for recurrence.Persistent hyperglycemia continuously activates pro-inflammatory pathways and reduces the capacity for mucosal repair, resulting in a higher likelihood of recurrent and prolonged infections following CDI.5,18
The high incidence and recurrence of CDI in diabetic patients are attributable not only to intrinsic immune and inflammatory mechanisms, but also to the additive effects of external factors such as clinical treatments and hospitalizations.Identifying and intervening in these high-risk factors is of great importance for optimizing CDI prevention and control strategies and improving outcomes in diabetic populations.1,5,16–18
Key Molecular Mechanisms, Potential Pathways, and Frontier Advances
Multiple basic and translational studies have revealed several key molecular mechanisms and signaling pathways by which diabetes promotes C. difficile infection (CDI) and its recurrence.A hyperglycemic environment can modulate innate immune recognition pathways such as Toll-like receptors (TLRs) and NOD-like receptors (NLRs), inducing sustained activation of intestinal mucosal inflammasomes (such as the NLRP3 inflammasome). This results in excessive secretion of pro-inflammatory factors such as IL-1β, IL-6, and TNF-α, which aggravate local and systemic inflammatory responses, disrupt intestinal barrier function, and provide favorable conditions for the colonization and toxin dissemination of C. difficile.18,19,21–29
Diabetes-related gut microbiota dysbiosis is characterized by a significant reduction in protective bacterial populations (such as Firmicutes and short-chain fatty acid–producing bacteria), while pathogenic bacteria like C. difficile and their related virulence factors are upregulated. Specifically, recent studies have found that patients with type 2 diabetes show increased abundances of opportunistic pathogens, such as Escherichia coli, Enterococcus, and Klebsiella species, and a marked reduction in butyrate-producing bacteria, including Faecalibacterium prausnitzii, Roseburia spp., and Eubacterium rectale, compared with non-diabetic individuals. These changes are associated with impaired intestinal barrier function and greater susceptibility to CDI.30 Short-chain fatty acids (such as butyrate) play a key role in maintaining the intestinal barrier and inhibiting the growth of pathogenic bacteria.In diabetic patients, the ability to synthesize short-chain fatty acids is diminished, resulting in weakened intestinal defense capability.17–19,31–33 Microbial metabolites (such as secondary bile acids and indole compounds) are closely related to the survival and pathogenicity of C. difficile.Under diabetic conditions, disturbances in these metabolites provide a suitable environment for C. difficile colonization.32–43
At the signaling pathway level, the sustained release of inflammatory factors amplifies the inflammatory cascade through pathways such as NF-κB and MAPK, while also damaging the tight junction proteins of intestinal epithelial cells (such as occludin and claudin), which further promotes the translocation of pathogens and toxins. In diabetic patients, the expression of antimicrobial peptides (such as defensins and cathelicidins) is downregulated, reducing the direct defensive capability of the intestinal mucosa.18,19,21–26
In terms of frontier interventions, fecal microbiota transplantation (FMT), supplementation with probiotics or synbiotics, and small-molecule drugs targeting anti-inflammatory pathways have all shown potential to improve gut microbiota and reduce CDI susceptibility and recurrence rates in both diabetic and CDI animal models as well as in preliminary clinical studies.18 Small-molecule inhibitors targeting signaling pathways such as NLRP3 and NF-κB, and novel biologics such as IL-1β antagonists, have also provided new strategies for CDI prevention and control in high-risk patients.21–27
The molecular network of the diabetes–gut–inflammation axis represents an important research direction for precision prevention and control among high-risk populations for CDI in the future.In-depth elucidation of these molecular mechanisms will help promote translational applications from basic research to clinical practice, providing theoretical support and intervention targets for developing individualized and targeted prevention strategies.
Antibiotic Stewardship and Prevention Strategies
Antibiotic exposure is widely recognized as the single most important modifiable risk factor for the development and recurrence of C. difficile infection (CDI), particularly among high-risk populations such as patients with diabetes. Our findings underscore the need for robust antibiotic stewardship programs, which have been shown to significantly reduce CDI incidence in both hospital and community settings.
A meta-analysis of stewardship interventions demonstrated that restricting unnecessary use of broad-spectrum antibiotics—including clindamycin, cephalosporins, and fluoroquinolones—can lead to substantial reductions in CDI rates among hospitalized patients.44 Another systematic review and meta-analysis found that antibiotic stewardship, particularly when combined with infection prevention measures, resulted in an approximate 32% decrease in hospital-acquired CDI incidence.45 The Infectious Diseases Society of America (IDSA) and the Society for Healthcare Epidemiology of America (SHEA) also highlight reduction of CDI as one of the principal benefits of implementing antimicrobial stewardship programs.46
For diabetic patients, integrating antibiotic stewardship with individualized infection control and optimal diabetes management may provide the greatest benefit in preventing CDI and improving clinical outcomes.In summary, the combination of targeted antibiotic stewardship and comprehensive risk factor management represents an essential pathway for reducing the burden of CDI, particularly in vulnerable groups such as those with diabetes.
According to current clinical guidelines, fidaxomicin and vancomycin are recommended as the preferred first-line agents for CDI treatment, with metronidazole reserved for non-severe cases if other options are unavailable. Fidaxomicin has been shown to have similar efficacy as vancomycin, but with a lower risk of recurrence.However, in China, fidaxomicin is not yet widely available, and vancomycin and metronidazole remain the primary treatment options in most hospitals due to cost and accessibility constraints. Fecal microbiota transplantation (FMT) is considered for patients with multiple recurrences or those who fail antibiotic therapy.30
In China, vancomycin and metronidazole are the primary antibiotics used for the treatment of CDI, as fidaxomicin is not yet widely available due to cost and accessibility limitations.Vancomycin is generally recommended as the first-line agent for moderate-to-severe CDI, while metronidazole is reserved for mild cases or as an alternative when vancomycin is not available.Although fidaxomicin is recommended by international guidelines for its efficacy and lower recurrence rate, its routine clinical use remains rare in most Chinese hospitals.
For patients with multiple recurrences of CDI who do not respond to standard antibiotic therapy, fecal microbiota transplantation (FMT) has emerged as an effective salvage therapy. In recent years, FMT has become increasingly available in large tertiary hospitals in China, though its overall utilization is still limited due to resource and regulatory constraints.
In addition to current antibiotic and FMT therapies, novel treatment approaches such as the monoclonal antibody bezlotoxumab, bacteriophage therapy, tailocins, and antibacterial peptides have shown promise in reducing CDI recurrence and improving outcomes, especially in high-risk populations like patients with diabetes.Further research and clinical trials are ongoing to determine the effectiveness and feasibility of these new therapies.47
Clinical Implications for Management and Infection Control
The results of this study indicate that diabetic patients represent a classic high-risk group for both the initial onset and recurrence of C. difficile infection (CDI), which places higher demands on clinical management and infection control. In clinical practice, diabetic patients should be regarded as a priority population for CDI screening and prevention, especially during hospitalization or when receiving high-risk medications such as antibiotics or proton pump inhibitors (PPIs).Risk assessment and early warning should be strengthened during these periods. For diabetic patients with a history of CDI or combined factors such as advanced age, immunosuppression, or renal insufficiency, regular monitoring of gastrointestinal symptoms is needed to enable early identification and timely intervention.
Antibiotic stewardship is a key component in the prevention and control of CDI. It is essential to strictly implement principles of rational antibiotic use among diabetic patients, avoiding the misuse of broad-spectrum antibiotics and combination therapies. When necessary, consultation with an antimicrobial stewardship (AMS) team should be conducted to balance infection control with the management of underlying diseases.For patients requiring long-term PPI therapy, indications should be regularly reviewed to reduce unnecessary use of gastric acid suppressants, thereby lowering the risk of CDI at its source.19
Protection and intervention of the gut microbiota are also important strategies. For diabetic patients, early supplementation with probiotics or synbiotics during antibiotic therapy or hospitalization can be considered to maintain the diversity of the gut microbiota and enhance intestinal barrier function. For patients at high risk of recurrence, innovative microbiota-based therapies such as fecal microbiota transplantation (FMT) can serve as second- or third-line interventions.Multiple current guidelines and evidence-based studies have shown that FMT can significantly reduce the recurrence rate of CDI.18
Comprehensive management of diabetic patients’ basic metabolism, immune function, and nutritional status should also be strengthened, including optimizing blood glucose control, preventing chronic complications, and engaging in appropriate physical exercise, in order to indirectly improve the overall defense capability against infections.Hospitals and long-term care institutions should develop individualized infection control measures for diabetic patients, such as environmental cleaning, contact isolation, and education of healthcare staff, to reduce the risk of nosocomial transmission and recurrence.
In summary, the prevention and control of CDI in diabetic patients requires an integrated approach involving antibiotic stewardship, maintenance of the gut microbiota, metabolic interventions, and multidisciplinary collaboration, shifting from single-disease management to comprehensive risk control throughout the disease course .In the future, enhanced screening, follow-up, and targeted interventions for high-risk populations should be promoted, facilitating the translation of evidence into daily clinical practice to ultimately improve the health outcomes of diabetic patients with CDI.5,16
Considering clinical realities in China, the prevention and control of CDI in diabetic patients should also focus on local high-risk factors and population characteristics. In China, the rates of antibiotic and PPI use are high, and there is a large population of elderly diabetic patients with multiple comorbidities, making infection control even more complex. It is recommended to further standardize the use of high-risk medications in clinical practice, strengthen microbiota-based interventions (such as probiotics and fecal microbiota transplantation), and promote multicenter prospective cohort studies to establish risk prediction and management models specific to CDI in the Chinese population. In the future, more emphasis should also be placed on patient and healthcare provider education, multidisciplinary teamwork, and data sharing to enhance the comprehensive prevention and control of CDI in diabetic patients, thereby contributing Chinese experience to the global effort against C. difficile infection.
Strengths and Limitations of the Study with Dual Primary Outcomes
This study used the risk of CDI occurrence and recurrence as dual primary outcomes to systematically assess the impact of diabetes on the entire course of C. difficile infection, comprehensively elucidating the clinical significance of diabetes in CDI prevention and control. The research integrated large-sample cohort and case-control studies from multiple countries and regions, applying strict inclusion criteria to ensure the representativeness and generalizability of the results.
Several limitations should be noted. First, all studies included in this analysis were observational in nature, making it difficult to fully rule out the influence of confounding factors.Second, most included studies did not specify whether patients had type 1 or type 2 diabetes, and the majority of participants were adults who were likely to have type 2 diabetes.However, due to the lack of separate data, subgroup analysis by diabetes type could not be conducted.This limitation may reduce the precision of the results and highlights the need for future studies to report and analyze diabetes subtypes separately. Third, there were variations across different studies in the definitions of diabetes and CDI, as well as in variable adjustment methods, which may affect the accuracy of effect estimates. Fourth, for certain outcomes such as the risk of CDI recurrence, the number of included studies was relatively limited and some studies had small sample sizes, resulting in limited statistical power.Publication bias may also exist due to missing original data. In addition, the restriction to English-language publications may have introduced language bias.Finally, moderate to high heterogeneity was observed in some subgroup and overall analyses, suggesting that regional, population, and methodological differences may affect the interpretation of the results.In addition, limited information was available in many included studies regarding the specific antibiotic treatments (particularly fidaxomicin and vancomycin) received by patients, making it difficult to evaluate the influence of these recommended therapies on outcomes.
Therefore, further high-quality, prospective, multicenter studies with larger sample sizes and standardized reporting—particularly those that distinguish between type 1 and type 2 diabetes—are needed to supplement and validate our conclusions and to enhance the robustness and clinical relevance of the evidence.
Conclusion
This study assessed the association between diabetes and C. difficile infection (CDI), and the results showed that diabetic patients have a moderately elevated risk of both initial and recurrent CDI compared to non-diabetic populations. These findings suggest that diabetes should be regarded as a key target population for CDI prevention and control. In clinical practice, it is necessary to strengthen risk identification, ensure the rational use of antibiotics, and optimize gut microbiota management for diabetic patients. Further high-quality, prospective studies are needed to clarify the underlying mechanisms and optimize intervention strategies, with the goal of comprehensively improving infection prevention and health outcomes in diabetic patients.
In addition to current standard treatments, emerging approaches such as monoclonal antibodies, bacteriophages, tailocins, and antibacterial peptides may offer promising options for the future management of CDI, particularly in high-risk groups like those with diabetes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sharma S, Weissman S, Walradt T, et al. Readmission, healthcare consumption, and mortality in Clostridium difficile infection hospitalizations: a nationwide cohort study. Int J Colorectal Dis. 2021;36(12):2629–2635. doi:10.1007/s00384-021-04001-w
2. Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile infection in the United States. N Engl J Med. 2015;372(9):825–834. doi:10.1056/NEJMoa1408913
3. Jin K, Li J, Liu L, et al. Molecular epidemiology of Clostridium difficile infection in hospitalized patients in eastern China. J Med Microbiol. 2017;66(11):1626–1634. doi:10.1099/jmm.0.000617
4. Guh AY, Kutty PK. Clostridioides difficile infection. Ann Intern Med. 2018;169(7):
5. López-de-Andrés A, Esteban-Vasallo MD, De Miguel-Díez J, et al. Incidence and in-hospital outcomes of Clostridium difficile infection among type 2 diabetes patients in Spain. Int J Clin Pract. 2018;72(10):e13251. doi:10.1111/ijcp.13251
6. Zhang Y, Shaikh N, Ferey JL, et al. Lactotrehalose, an analog of trehalose, increases energy metabolism without promoting Clostridioides difficile infection in mice. Gastroenterology. 2020;158(5):1402–1416.e2. doi:10.1053/j.gastro.2019.11.295
7. Wong-McClure RA, Ramírez-Salas E, Mora-Brenes N, et al. Long term effect of infection control practices and associated factors during a major Clostridium difficile outbreak in costa rica. J Infect Dev Ctries. 2013;7(12):914–921. doi:10.3855/jidc.2854
8. Aseeri M, Schroeder T, Kramer J, Zackula R. Gastric acid suppression by proton pump inhibitors as a risk factor for Clostridium difficile -associated diarrhea in hospitalized patients. Am J Gastroenterol. 2008;103(9):2308–2313. doi:10.1111/j.1572-0241.2008.01975.x
9. Basturk T, Albayrak R, Ulas T, et al. Evaluation of resistive index by color doppler imaging of orbital arteries in type ii diabetes mellitus patients with microalbuminuria. Renal Failure. 2012;34(6):708–712. doi:10.3109/0886022X.2012.672266
10. Dimitrova G. Relation between retrobulbar circulation and progression of diabetic retinopathy. Br J Ophthalmol. 2003;87(5):622–625. doi:10.1136/bjo.87.5.622
11. Linney S, Fernandes T, Einarson T, Sengar A, Walker JH, Mills A. Association between use of proton pump inhibitors and a Clostridium difficile -associated disease outbreak: case-control study. CJHP. 2010;63(1):31–37. doi:10.4212/cjhp.v63i1.866
12. Xiao Y, Wang J, Shen P, et al. Ten years of surveillance of antibiotic consumption in China, 2010–2019. J Antimicrob Chemother. 2022;77(3):803–813. doi:10.1093/jac/dkab457
13. Zarowitz BJ, Allen C, O’Shea T, Strauss ME. Risk factors, clinical characteristics, and treatment differences between residents with and without nursing home- and non-nursing home-acquired Clostridium difficile Infection. JMCP. 2015;21(7):585–595. doi:10.18553/jmcp.2015.21.7.585
14. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
15. Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. doi:10.1136/bmj.i4919
16. Olanipekun TO, Salemi JL, Mejia De Grubb MC, Gonzalez SJ, Zoorob RJ. Clostridium difficile infection in patients hospitalized with type 2 diabetes mellitus and its impact on morbidity, mortality, and the costs of inpatient care. Diabetes Res Clin Pract. 2016;116:68–79. doi:10.1016/j.diabres.2016.04.021
17. Kumar A, Teslova T, Taub E, Miller JD, Lukin DJ. Comorbid diabetes in inflammatory bowel disease predicts adverse disease-related outcomes and infectious complications. Dig Dis Sci. 2021;66(6):2005–2013. doi:10.1007/s10620-020-06439-4
18. Bakker GJ, Nieuwdorp M. Fecal microbiota transplantation: therapeutic potential for a multitude of diseases beyond Clostridium difficile. Britton RA, Cani PD. editors. Microbiol Spectr. 2017;5(4)
19. Game F. Management of osteomyelitis of the foot in diabetes mellitus. Nat Rev Endocrinol. 2010;6(1):43–47. doi:10.1038/nrendo.2009.243
20. Darwitz R, Bohnsack JF, Thurlow LR, et al. Triple threat: how diabetes results in worsened bacterial infections. Infect Immun. 2024;92(9):e0050923. doi:10.1128/iai.00509-23
21. Rodrigues MA, Brady RR, Rodrigues J, Graham C, Gibb AP. Clostridium difficile infection in general surgery patients; identification of high-risk populations. Int J Surg. 2010;8(5):368–372. doi:10.1016/j.ijsu.2010.05.004
22. Rzucidło-Hymczak A, Hymczak H, Olechowska-Jarząb A, et al. Clostridioides difficile infection after cardiac surgery: assessment of prevalence, risk factors and clinical outcomes—retrospective study. PeerJ. 2020;8:e9972. doi:10.7717/peerj.9972
23. Ro Y, Eun CS, Kim HS, et al. Risk of Clostridium difficile infection with the use of a proton pump inhibitor for stress ulcer prophylaxis in critically Ill patients. Gut Liver. 2016;10(4):581–586. doi:10.5009/gnl15324
24. Al-Mazrou AM, Hyde LZ, Suradkar K, Kiran RP. Effect of inclusion of oral antibiotics with mechanical bowel preparation on the risk of Clostridium difficile infection after colectomy. J Gastrointestinal Surg. 2018;22(11):1968–1975. doi:10.1007/s11605-018-3837-3
25. Kassam Z, Cribb Fabersunne C, Smith MB, et al. Clostridium difficile associated risk of death score (CARDS): a novel severity score to predict mortality among hospitalised patients with C. difficile infection. Aliment Pharmacol Ther. 2016;43(6):725–733. doi:10.1111/apt.13546
26. Stewart DB, Hollenbeak CS. Clostridium difficile colitis: factors associated with outcome and assessment of mortality at a national level. J Gastrointestinal Surg. 2011;15(9):1548–1555. doi:10.1007/s11605-011-1615-6
27. Mi H, Bao R, Xiao Y, et al. Colonization of toxigenic Clostridium difficile among intensive care unit patients: a multi-centre cross-sectional study. Front Cell Infect Microbiol. 2020;10:12. doi:10.3389/fcimb.2020.00012
28. Fujioka S, Karashima K, Nishikawa N, Saito Y. Correlation between higher blood flow velocity in the central retinal vein than in the central retinal artery and severity of nonproliferative diabetic retinopathy. Jpn J Ophthalmol. 2006;50(4):312–317. doi:10.1007/s10384-005-0338-1
29. Kanagaraju V, Divya K, Raajaganesh M, Devanand B. Evaluation of resistive index of orbital vessels using color doppler imaging in patients with type 2 diabetes mellitus. J Med Ultrasound. 2021;29(2):111–115. doi:10.4103/JMU.JMU_88_20
30. Młynarska E, Grywalska E, Mielcarska MB, et al. Exploring the significance of gut microbiota in diabetes pathogenesis and management—a narrative review. Nutrients. 2024;16(12):1938. doi:10.3390/nu16121938
31. Moon CM, Hong SN. Fecal microbiota transplantation beyond Clostridioides difficile infection. Clin Endosc. 2021;54(2):149–151. doi:10.5946/ce.2021.068
32. Çekiç O, Bardak Y, Tığ ŞU, et al. Hemodynamic response to intravitreal triamcinolone in eyes with macular edema: intravitreal triamcinolone and ocular blood flow. Int Ophthalmol. 2007;27(5):313–319. doi:10.1007/s10792-007-9080-7
33. Chalew S, Gomez R, Vargas A, et al. Hemoglobin A1c, frequency of glucose testing and social disadvantage: metrics of racial health disparity in youth with type 1 diabetes. J Diabet Complicat. 2018;32(12):1085–1090. doi:10.1016/j.jdiacomp.2018.02.008
34. Neroev VV, Kiseleva TN, Okhotsimskaya TD, Fadeeva VA, Ramasanova KA. Impact of antiangiogenic therapy on ocular blood flow and microcirculation in diabetic macular edema. Vestn oftal’mol. 2018;134(4):3. doi:10.17116/oftalma20181340413
35. Shahin M, Gad MA, Hamza W. Impact of intravitreal triamcinolone acetonide versus intravitreal bevacizumab on retrobulbar hemodynamic in patients with diabetic macular edema. Cutaneous Ocular Toxicol. 2014;33(1):49–53. doi:10.3109/15569527.2013.796478
36. Alicino C, Giacobbe DR, Durando P, et al. Increasing incidence of Clostridium difficile infections: results from a 5-year retrospective study in a large teaching hospital in the Italian region with the oldest population. Epidemiol Infect. 2016;144(12):2517–2526. doi:10.1017/S0950268816000935
37. Farooq U, Tarar ZI, Kamal F, Malik A, Bresnahan J, Abegunde AT. Is acid suppression associated with the increased length of stay in diabetic ketoacidosis patients? A nationwide analysis. J Intern Med. 2022;292(1):136–145. doi:10.1111/joim.13466
38. Papić N, Jelovčić F, Karlović M, Marić LS, Vince A. Nonalcoholic fatty liver disease as a risk factor for Clostridioides difficile infection. Eur J Clin Microbiol Infect Dis. 2020;39(3):569–574. doi:10.1007/s10096-019-03759-w
39. Rattan R, Allen CJ, Sawyer RG, et al. Patients with risk factors for complications do not require longer antimicrobial therapy for complicated intra-abdominal infection. American Surg. 2016;82(9):860–866. doi:10.1177/000313481608200951
40. Eliakim-Raz N, Fishman G, Yahav D, et al. Predicting Clostridium difficile infection in diabetic patients and the effect of metformin therapy: a retrospective, case–control study. Eur J Clin Microbiol Infect Dis. 2015;34(6):1201–1205. doi:10.1007/s10096-015-2348-3
41. Moayyedi P, Eikelboom JW, Bosch J, et al. Safety of proton pump inhibitors based on a large, multi-year, randomized trial of patients receiving rivaroxaban or aspirin. Gastroenterology. 2019;157(3):682–691.e2. doi:10.1053/j.gastro.2019.05.056
42. Amjad W, Qureshi W, Malik A, Singh R, Jafri S. The outcomes of Clostridioides difficile infection in inpatient liver transplant population. Transplant Infectious Dis. 2022;24(1):e13750. doi:10.1111/tid.13750
43. Rogozin E, Maree H, Masarwi M, et al. Usage of oral vancomycin for acute Clostridioides difficile infection (CDI) resulting in later acquisitions of vancomycin-resistant enterococci (VRE). Infect Control Hosp Epidemiol. 2025;46(7):703–709. doi:10.1017/ice.2025.81
44. Feazel LM, Malhotra A, Perencevich EN, Kaboli P, Diekema DJ, Schweizer ML. Effect of antibiotic stewardship programmes on Clostridium difficile incidence: a systematic review and meta-analysis. J Antimicrob Chemother. 2014;69(7):1748–1754. doi:10.1093/jac/dku086
45. Baur D, Gladstone BP, Burkert F, et al. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: a systematic review and meta-analysis. Lancet Infect Dis. 2017;17(9):990–1001. doi:10.1016/S1473-3099(17)30325-0
46. Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an antibiotic stewardship program: guidelines by the infectious diseases society of America and the society for healthcare epidemiology of America. Clin Infect Dis. 2016;62(10):e51–e77. doi:10.1093/cid/ciw118
47. Bratkovič T, Skok B, Jerala R, et al. New treatment approaches for Clostridioides difficile infections: alternatives to antibiotics and fecal microbiota transplantation. Gut Microbes. 2024;16(1):2337312. doi:10.1080/19490976.2024.2337312
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Update on the Role and Potential Molecules in Relation to Ruminococcus gnavus in Inflammatory Bowel Disease, Obesity and Diabetes Mellitus

Hong J, Fu T, Liu W, Du Y, Bu J, Wei G, Yu M, Lin Y, Min C, Lin D
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1235-1248
Published Date: 11 March 2024
Diabetes Mellitus Negatively Impacts Outcomes of HBV-Related Hepatocellular Carcinoma Following Thermal Ablation
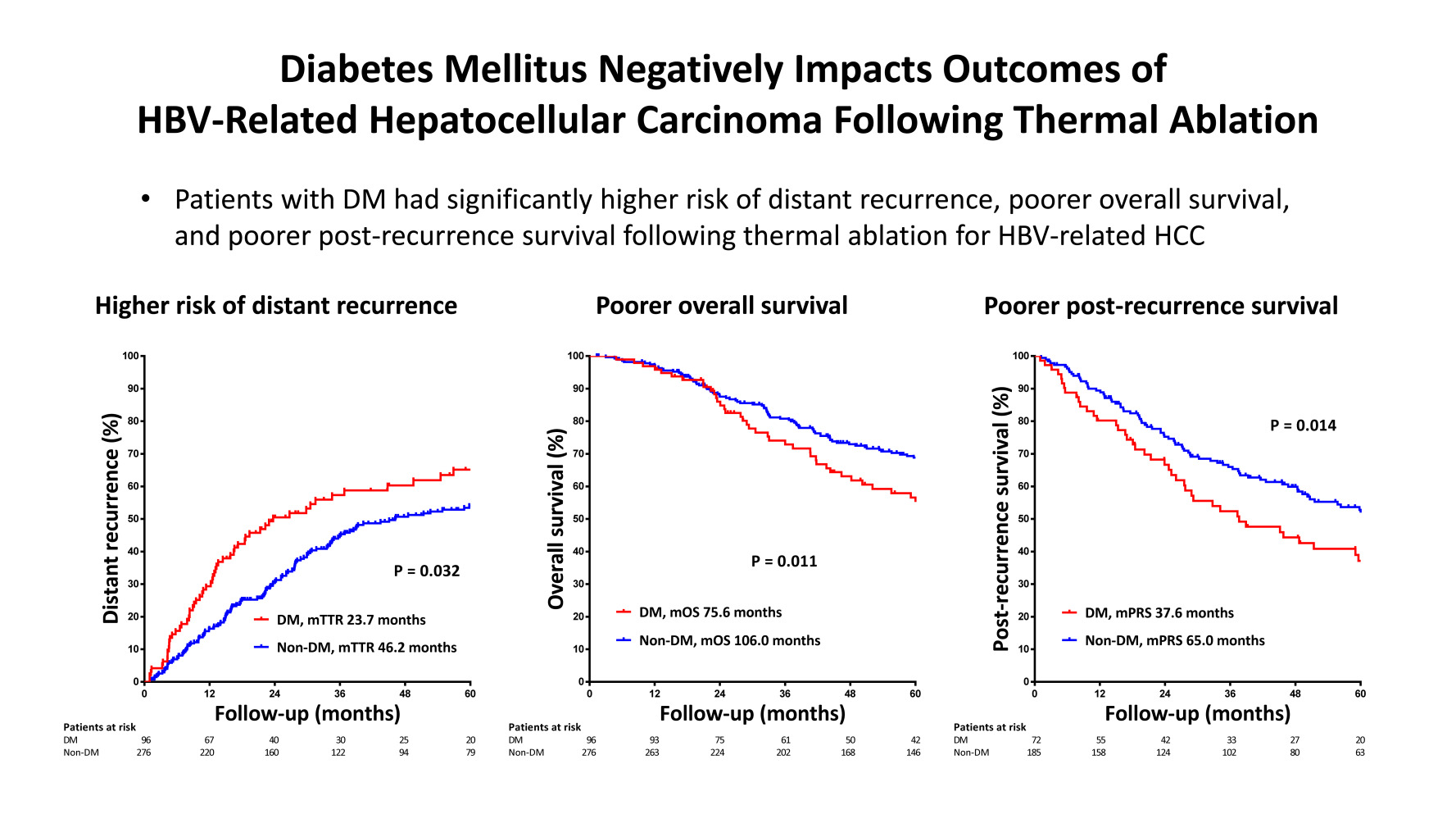
Wu KC, Lee IC, Liu CA, Chiu NC, Hsu SJ, Lee PC, Wu CJ, Chi C, Luo JC, Hou MC, Huang YH
Journal of Hepatocellular Carcinoma 2024, 11:2257-2267
Published Date: 19 November 2024