Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Metabolic Crosstalk in Diabetic Kidney Disease: Synergistic Effects of Glucotoxicity and Lipotoxicity
Authors Cao J, Dun Z, Tian D, Qiao Z, Wang Y
Received 12 November 2025
Accepted for publication 13 March 2026
Published 23 March 2026 Volume 2026:19 580866
DOI https://doi.org/10.2147/DMSO.S580866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Junying Cao,1 Zhihua Dun,1 Dandan Tian,1 Zhihui Qiao,1 Yuehua Wang1,2
1The Second Affiliated Hospital of Hebei University of Chinese Medicine (Hebei Province Seventh People’s Hospital), Dingzhou, Hebei, 073000, People’s Republic of China; 2College of Integrated Chinese and Western Medicine, Hebei University of Chinese Medicine, Shijiazhuang, Hebei, 050200, People’s Republic of China
Correspondence: Yuehua Wang, College of Integrated Chinese and Western Medicine, Hebei University of Chinese Medicine, No. 3 Xingyuan Road, Shijiazhuang, Hebei, 050200, People’s Republic of China, Email [email protected]
Abstract: Diabetic kidney disease (DKD) affects approximately 40% of patients with diabetes and remains the leading cause of end-stage renal disease globally, posing a critical public health challenge. While hyperglycemia has long been considered the primary driver, the persistence of residual renal risk despite intensive glycemic control highlights a critical gap in our understanding of the disease’s multifaceted metabolic origins. This review addresses this gap by shifting the focus beyond the “gluco-centric” paradigm to the synergistic lethality of “glucolipotoxicity.” We synthesize evidence showing how insulin resistance acts as a central hub connecting glucotoxicity and lipotoxicity, triggering a self-perpetuating vicious cycle of injury. Specifically, we dissect the molecular crosstalk across key pathogenic nodes, including the TXNIP-mTOR axis suppressing autophagy, DAG-PKC signaling driving insulin resistance, and the activation of the NLRP3 inflammasome. These intersecting pathways converge to accelerate oxidative stress, mitochondrial dysfunction, and fibrosis. We conclude by discussing the clinical implications of this metabolic framework, emphasizing how emerging multi-target therapies, such as SGLT2 inhibitors and GLP-1 receptor agonists, offer a translational pathway from mechanistic insights to precision medicine for preserving renal function.
Keywords: diabetic kidney disease, glucolipotoxicity, insulin resistance, lipotoxicity, oxidative stress
Introduction
Diabetic kidney disease (DKD), a critical microvascular complication of diabetes, has solidified its position as the primary driver of chronic kidney disease (CKD) and the leading cause of kidney failure with replacement therapy (KFRT) globally, presenting a formidable challenge to public health systems.1,2 The most recent epidemiological analyses, utilizing data from the Global Burden of Disease (GBD) 2023 study, reveal that CKD affects over 10% of the world’s population.3 Within this expansive patient population, DKD remains the predominant contributor, responsible for approximately 48.6% of all cases of KFRT.2 Furthermore, the global burden of diabetes-related CKD has exhibited a relentless upward trajectory over the past three decades and is projected to escalate further, particularly in regions with lower sociodemographic indexes.4,5
For many years, a “gluco-centric” view positioned hyperglycemia as the solitary pathogenic driver of DKD. However, this paradigm has been challenged by compelling evidence from both clinical trials and basic research, which shows that intensive glycemic control alone is often insufficient to halt the progression of renal damage.6 This has necessitated a shift in perspective, bringing the critical role of lipid dysregulation into sharp focus as an independent and pivotal factor.7 The kidney is not merely a passive victim but an active participant in lipid metabolism. In the diabetic state, renal cells, including podocytes and tubular epithelial cells, develop a significant intracellular accumulation of lipids—a condition termed renal lipotoxicity, which can independently trigger inflammation, fibrosis, and cellular dysfunction.8 Therefore, the central problem this review seeks to address is the dissection of the synergistic and often overlooked interplay between glucotoxicity and lipotoxicity in driving DKD progression. While the detrimental effects of hyperglycemia are well-established, the precise molecular mechanisms linking it to subsequent renal lipid dysregulation remain an area of intense investigation and some controversy.9,10
When the toxic effects of elevated glucose (glucotoxicity) and dysregulated lipids (lipotoxicity) converge within the renal microenvironment, their detrimental impact is not merely additive but synergistic—a phenomenon now recognized as glucolipotoxicity.11 This concept is fundamental to understanding the cellular basis of DKD, as the molecular crosstalk between glucose and lipid metabolic pathways collaboratively amplifies intracellular damage. Specifically, hyperglycemia can actively drive de novo lipogenesis and disrupt fatty acid oxidation within renal cells through pathways involving SREBPs and ChREBP.7 This synergy exacerbates endoplasmic reticulum and oxidative stress, activates potent inflammatory signaling pathways such as the NLRP3 inflammasome, and ultimately precipitates mitochondrial dysfunction and apoptosis in critical renal cells, including podocytes and tubular epithelial cells.12,13 This creates a self-perpetuating cycle of injury that accelerates the progression from early glomerular damage to terminal sclerosis and fibrosis.
The common upstream driver that intricately links these dual metabolic insults is insulin resistance, which acts as the central hub connecting dysregulated glucose and lipid metabolism in DKD. Recent research, spanning from 2022 to 2025, continues to reinforce this concept, highlighting that insulin resistance, even preceding overt hyperglycemia, can initiate renal damage by promoting inflammation through TLR4 activation and directly impairing insulin signaling in podocytes and glomerular endothelial cells.14–16 The integrity of insulin signaling is crucial for the normal function of renal cells. When this signaling is impaired, it not only causes direct cellular dysfunction—such as podocyte effacement—but also disrupts intracellular lipid mediator pathways, firmly coupling glucotoxicity with lipotoxicity.17 Furthermore, systemic insulin resistance promotes DKD progression through a multitude of parallel mechanisms, including the induction of chronic inflammation, oxidative stress, and adverse renal hemodynamics.18
Therefore, a comprehensive understanding of DKD pathogenesis requires a holistic approach that moves beyond a single-pathway focus. This review will critically synthesize the current knowledge on this dual pathological mechanism. It will first provide an updated overview of the key molecular players connecting glucose and lipid metabolism. Subsequently, it will delve into the central role of insulin resistance as the integrating hub for these metabolic insults. Finally, it will explore the downstream common pathways of inflammation and oxidative stress, and discuss how this integrated understanding is shaping current and emerging therapeutic strategies that target this metabolic vicious cycle.
Literature Search Strategy and Selection Criteria
To ensure a comprehensive and unbiased overview of the current understanding of DKD pathogenesis, we adopted a structured literature search strategy. This review focuses on the complex interplay between glucose and lipid metabolic disorders, while also systematically examining downstream pathways such as inflammation, oxidative stress, and autophagy to provide a balanced perspective.
Search Strategy and Data Sources
We conducted a systematic search of major electronic databases, including PubMed/MEDLINE, Embase, and Web of Science, covering the period from inception to December 2025. The search strategy employed a combination of Medical Subject Headings (MeSH) and free-text terms related to the following domains: (1) Disease context: “Diabetic Kidney Disease”, “Diabetic Nephropathy”, “Chronic Kidney Disease in Type 2 Diabetes”; (2) Metabolic drivers: “Glucotoxicity”, “Hyperglycemia”, “Lipotoxicity”, “Lipid metabolism”, “Fatty acid oxidation”, “Insulin resistance”; and (3) Pathogenic mechanisms: “Metabolic crosstalk”, “Oxidative stress”, “Inflammation”, “NLRP3 inflammasome”, “Autophagy”, “Mitophagy”, “Fibrosis”. Boolean operators (AND, OR) were used to combine these terms effectively. To ensure the inclusion of emerging evidence, we also manually screened the reference lists of identified relevant reviews and key primary studies.
Inclusion and Exclusion Criteria
The selection of studies was guided by pre-defined criteria to minimize selection bias. Inclusion criteria: (1) Peer-reviewed original research articles (in vitro, in vivo animal models, and clinical studies) and high-quality reviews; (2) Studies explicitly investigating the molecular mechanisms linking glucose or lipid metabolism to renal injury; (3) Articles published in the English language. Exclusion criteria: (1) Studies focusing solely on non-diabetic kidney diseases; (2) Purely epidemiological reports lacking mechanistic insights; (3) Editorials, conference abstracts, and case reports; (4) Studies with insufficient data or unclear methodology.
Data Screening and Synthesis
Initial screening was performed based on titles and abstracts to exclude irrelevant studies. Full-text articles of potentially relevant citations were then retrieved and assessed against the inclusion criteria. Given the significant heterogeneity in study designs (ranging from molecular cell biology to clinical trials), a formal meta-analysis was not feasible. Instead, a narrative synthesis approach was employed. Ultimately, 94 studies meeting the quality and relevance criteria were included in this review (Figure 1). This structured approach ensures that the review reflects the broad spectrum of existing literature, encompassing both established paradigms and emerging alternative pathways.
 |
Figure 1 Flowchart of literature search and screening strategy. |
Glucose Metabolism Disorder and Diabetic Kidney Disease (DKD)
Hyperglycemia is the primary initiator of the metabolic disturbances that characterize DKD. The persistent excess of glucose overwhelms normal metabolic pathways in the kidney, triggering a complex network of cellular stress responses that drive renal injury. This process involves the overactivation of damaging biochemical routes, the development of renal insulin resistance, and a profound reprogramming of cellular energy metabolism, which collectively promote glomerulosclerosis and tubulointerstitial fibrosis.19
Abnormal Glucose Metabolism and DKD
Chronic hyperglycemia directly inflicts damage upon renal cells through several interconnected pathways, most notably the formation of advanced glycation end-products (AGEs) and the flux through the polyol pathway. In glomerular cells, hyperglycemia fosters a pro-inflammatory and pro-sclerotic environment. Mesangial cells, when exposed to high glucose, increase their production of extracellular matrix components like type IV collagen and fibronectin, leading to mesangial expansion.20 Podocytes, the critical gatekeepers of the glomerular filtration barrier, undergo apoptosis and effacement of their foot processes under glycemic stress, a key event leading to the onset of albuminuria.21
The formation and accumulation of AGEs is a central mechanism of glucotoxicity. These products result from the non-enzymatic reaction of glucose with proteins, lipids, and nucleic acids. AGEs exert their detrimental effects either by direct cross-linking of matrix proteins—which increases stiffness and disrupts tissue architecture—or by engaging with their cell surface receptor (RAGE).22 The activation of the AGE-RAGE axis in podocytes and mesangial cells triggers intracellular signaling cascades, prominently involving NF-κB, which leads to the upregulation of pro-inflammatory cytokines and pro-fibrotic growth factors like TGF-β1, thereby perpetuating a cycle of inflammation and fibrosis.23,24 Recent high-quality evidence confirms that this signaling cascade induces podocyte dysfunction and promotes extracellular matrix deposition, directly contributing to glomerulosclerosis.25
Concurrently, the polyol pathway becomes pathologically active. In this route, aldose reductase converts excess glucose into sorbitol. The effects of this pathway can be distinguished as both acute and chronic. Acutely, the intracellular accumulation of sorbitol, particularly in cells with limited capacity to metabolize it, creates significant osmotic stress, leading to cellular swelling and dysfunction.26 Chronically, the pathway inflicts damage through two more insidious mechanisms. First, the conversion process consumes NADPH, an essential cofactor for regenerating the antioxidant glutathione, thus compromising the cell’s ability to counteract oxidative stress.27 Second, the subsequent oxidation of sorbitol to fructose alters the NAD+/NADH ratio, creating a state of “pseudohypoxia” that impairs the function of NAD+-dependent protective enzymes and further disrupts mitochondrial metabolism, causing direct damage to tubular structures.28
Impact of Insulin Resistance and Hyperinsulinemia on the Kidney
The kidney is a vital insulin-responsive organ, where insulin signaling is crucial for cell health. In podocytes, for instance, intact insulin signaling is essential for several key functions. It is necessary for cell survival, the proper maintenance of the actin cytoskeleton, and efficient autophagic function to clear damaged organelles.29 Consequently, the development of local insulin resistance disrupts these critical processes. This disruption leads directly to podocyte apoptosis and foot process effacement, which culminates in the breakdown of the glomerular filtration barrier and the onset of albuminuria.30
This cellular dysfunction is further compounded by a critical shift in energy metabolism, governed by the interplay between PGC-1α and HIF-1α. PGC-1α is the principal driver of mitochondrial biogenesis and FAO.31 In DKD, its expression is suppressed, leading to mitochondrial dysfunction, impaired FAO, and a cellular energy deficit.32,33 This forces a reliance on less efficient glycolysis. Concurrently, the diabetic kidney exists in a state of chronic local hypoxia, which activates HIF-1α. Chronic HIF-1α activation is maladaptive, promoting pro-inflammatory and pro-fibrotic gene expression.34 Recent studies have revealed a damaging crosstalk where activated HIF-1α directly inhibits PGC-1α transcriptional activity. This molecular “switch” effectively locks renal cells into a pathological state of low energy efficiency and high fibrotic signaling, accelerating the progression towards end-stage renal disease.35
Lipid Dysregulation and Diabetic Kidney Disease (DKD)
Building on the established role of glucotoxicity, the pathogenic landscape of DKD is profoundly shaped by a parallel and often intersecting process: lipid dysregulation.8,36 In the diabetic milieu, characterized by insulin resistance and systemic metabolic shifts, the kidney is exposed to and actively participates in a maladaptive lipid environment. This results in the intracellular accumulation of toxic lipid species within glomeruli and tubules, a condition known as renal lipotoxicity8 (Table 1).
 |
Table 1 Cell-Specific Responses to Glucolipotoxicity in the Diabetic Kidney |
Lipid Accumulation and Renal Lipotoxicity
The accumulation of lipids within the kidney is a central feature of DKD, arising from a dual insult: an increased influx of circulating lipids and an abnormal elevation of de novo lipogenesis within renal cells. In the context of diabetes and associated hyperlipidemia, kidney cells are overwhelmed by elevated levels of circulating free fatty acids (FFAs), leading to excessive uptake. This is not merely a feature of animal models; a substantial body of evidence confirms this in humans. Histological analyses of kidney biopsies from patients with DKD consistently show marked lipid droplet accumulation (via Oil Red O staining and electron microscopy) within glomerular and tubular cells.36 Furthermore, recent transcriptomic analyses of human DKD biopsies have corroborated these findings at a molecular level, revealing profound dysregulation of lipid metabolism pathways, including the upregulation of genes involved in lipid synthesis and uptake.41
Concurrently, the high-glucose and hyperinsulinemic state directly stimulates intra-renal lipid synthesis. A critical upstream regulator of this process is the mTORC1 signaling pathway, which, upon activation by metabolic excess, promotes the maturation and nuclear translocation of the master lipogenic transcription factor, Sterol Regulatory Element-Binding Protein-1c (SREBP-1c).42,43 Activated SREBP-1c, in turn, drives the transcriptional upregulation of crucial lipogenic enzymes like fatty acid synthase (FASN) and acetyl-CoA carboxylase (ACC), steering cellular metabolism towards the synthesis and storage of triglycerides, directly exacerbating the renal lipid burden.7
The resulting overload of specific lipid molecules incites lipotoxicity through distinct, cell-specific mechanisms. In podocytes, the accumulation of FFAs and cholesterol disrupts mitochondrial function and disorganizes the actin cytoskeleton, leading to foot process effacement and proteinuria.37 In renal tubular cells, the buildup of lipids such as triglycerides and ceramides is particularly damaging, triggering potent stress responses, including severe endoplasmic reticulum (ER) stress, heightened oxidative stress, and the activation of potent pro-inflammatory signaling cascades.8,38
Lipid Metabolism Remodeling and Functional Impairment
Beyond simple accumulation, lipotoxicity fundamentally remodels the kidney’s metabolic machinery. A critical aspect of this remodeling is the severe suppression of FAO, the primary energy-generating pathway in the high-demand renal tubular epithelial cells. The principal regulator of FAO, Peroxisome Proliferator-Activated Receptor alpha (PPARα), is consistently downregulated in the diabetic kidney. Mechanistic studies have established that this loss of PPARα activity is a causal driver of tubulointerstitial fibrosis, rather than a mere consequence, as restoring its signaling effectively mitigates renal injury.39 Building on this, landmark quantitative work has confirmed the severity of this defect, showing that the maximal rate of FAO can be reduced by over 50% in the tubular cells of diabetic kidneys compared to healthy controls.31
The consequences of impaired FAO are severe. It leads directly to a state of energy failure, compromising all tubular functions. Furthermore, the metabolic bottleneck in FAO causes the buildup of incompletely oxidized fatty acid intermediates, which generates excessive reactive oxygen species (ROS). This combination of energy depletion and severe oxidative stress is a potent trigger for tubular cell apoptosis and contributes directly to tubulointerstitial atrophy.31,39
The toxic intracellular environment also activates innate immune pathways. Lipids, particularly saturated fatty acids, can act as danger signals that trigger the assembly of the NLRP3 inflammasome. Activation of this complex leads to the release of potent pro-inflammatory cytokines, IL-1β and IL-18.44 This process establishes chronic inflammation and directly contributes to fibrosis, creating a vicious cycle of energy starvation, oxidative stress, and tissue damage central to DKD progression.45
The Vicious Cycle: Crosstalk Between Glucose and Lipid Metabolism in DKD
The preceding sections have delineated the independent pathogenic roles of disordered glucose and lipid metabolism in the progression of DKD. However, these pathways do not operate in isolation. Rather, they are deeply intertwined, engaging in a damaging crosstalk that establishes a self-perpetuating vicious cycle of cellular injury.46 This metabolic inflexibility, where renal cells can neither efficiently utilize glucose nor oxidize fatty acids, results in the accumulation of toxic metabolic intermediates, fueling a common downstream cascade of oxidative stress, inflammation, and fibrosis. Understanding the molecular nodes that connect these two metabolic arms is critical to appreciating the full complexity of DKD pathogenesis and identifying more effective therapeutic strategies46,47 (Table 2 and Figure 2).
 |
Table 2 Key Molecular Mediators in the Metabolic Crosstalk of Diabetic Kidney Disease |
 |
Figure 2 Schematic illustration of the vicious cycle linking disordered glucose and lipid metabolism in diabetic kidney disease (DKD). Persistent hyperglycemia and hyperlipidemia (elevated free fatty acids, FFAs) converge to induce insulin resistance, which serves as a central integrator disrupting both glucose and lipid homeostasis. Hyperglycemia drives transcriptional activation of de novo lipogenesis via ChREBP, fueling lipotoxicity characterized by lipid droplet accumulation and ceramide/diacylglycerol buildup, alongside impaired fatty acid oxidation (FAO) due to reduced PPARα activity. Concurrently, glucotoxicity involves activation of the advanced glycation end products (AGEs)/RAGE pathway and the polyol pathway. Both pathways collectively suppress autophagy through the TXNIP-mTOR axis, preventing clearance of damaged mitochondria and lipotoxic intermediates. This metabolic inflexibility exacerbates insulin resistance and increases hepatic gluconeogenesis, establishing a feed-forward loop that intensifies glucotoxicity. The combined glucolipotoxic environment activates chronic inflammation, as indicated by upregulation of the NLRP3 inflammasome and NF-κB signaling, alongside oxidative stress driven by increased NOX4/NOX5 activity and mitochondrial dysfunction producing reactive oxygen species (ROS). These processes synergistically elevate TGF-β1 signaling, which orchestrates renal fibrosis and injury hallmarked by glomerulosclerosis, tubulointerstitial fibrosis, and podocyte loss. This diagram encapsulates the intricate crosstalk and amplifying feedback mechanisms between disordered glucose and lipid metabolism that underpin the progression of DKD, highlighting molecular targets for therapeutic intervention. |
Insulin Resistance: The Core Integrator
Insulin resistance (IR) stands as the central hub integrating the dysregulation of both glucose and lipid homeostasis, creating the foundational conditions for gluco-lipotoxicity in the kidney. Systemically, IR disrupts glucose metabolism by impairing glucose uptake in peripheral tissues like muscle and adipose tissue while failing to suppress hepatic gluconeogenesis, thereby sustaining hyperglycemia.30 Simultaneously, IR unleashes a torrent of free fatty acids (FFAs) into circulation by promoting uncontrolled lipolysis in adipocytes. This elevated systemic availability of both glucose and FFAs places an immense metabolic burden on the kidney.30,60
Within the kidney itself, the development of local insulin resistance further amplifies cellular damage. Podocytes, for instance, rely on intact insulin signaling for survival and the maintenance of their intricate cytoarchitecture. Seminal studies using podocyte-specific insulin receptor knockout (PIRKO) mice have conclusively demonstrated that the loss of insulin signaling is sufficient to cause severe albuminuria and classic features of glomerulosclerosis, even in the absence of systemic hyperglycemia.21 In renal tubular cells, IR impairs their ability to adapt to metabolic stress, disrupting mitochondrial function and rendering them more susceptible to FFA-induced apoptosis. Thus, insulin resistance acts as the critical initiator, simultaneously creating the hyperglycemic and hyperlipidemic environment while disabling the cell’s intrinsic defense mechanisms, thereby setting the stage for renal decline.60,61
Hyperglycemia Fuels Lipid Dysregulation
Persistent hyperglycemia actively drives the accumulation of lipids within renal cells, directly transforming a glucose problem into a lipid problem. The primary mechanism for this is the transcriptional activation of de novo lipogenesis (DNL), the metabolic process of synthesizing fatty acids from non-lipid precursors. High intracellular glucose levels lead to an abundance of substrates like acetyl-CoA, which are channeled into lipid synthesis through the activation of the Carbohydrate-Responsive Element-Binding Protein (ChREBP).48
ChREBP acts as a master transcriptional regulator that senses high glucose levels and, in response, upregulates a suite of lipogenic genes, including fatty acid synthase (FASN) and acetyl-CoA carboxylase (ACC). Studies involving cultured human mesangial cells exposed to high glucose have demonstrated a marked induction of ChREBP and a subsequent increase in intracellular triglyceride content.49 This intra-renal lipid synthesis exacerbates the lipid burden delivered from the circulation, leading to significant lipid droplet accumulation, particularly within podocytes and tubular epithelial cells, driving lipotoxicity.
Furthermore, hyperglycemia disrupts cellular housekeeping mechanisms that would normally clear toxic aggregates, most notably autophagy. Autophagy is a critical process for degrading damaged organelles and misfolded proteins. In DKD, autophagic flux is significantly impaired. One key link between hyperglycemia and failed autophagy is the Thioredoxin-Interacting Protein (TXNIP). TXNIP expression is robustly induced by high glucose and serves as a major sensor of glucotoxicity.62 Specifically, high glucose-induced TXNIP acts as a direct upstream activator of the mammalian target of rapamycin (mTOR) complex 1 (mTORC1).50 This activation of mTORC1, a potent negative regulator of autophagy, subsequently suppresses the autophagic flux.51 By inhibiting mTORC1, either through TXNIP deficiency or pharmacological intervention, autophagy can be restored, highlighting the crucial role of the TXNIP-mTORC1 axis in linking hyperglycemia to impaired cellular clearance in DKD.52
Lipotoxicity Exacerbates Glucose Metabolic Disorders
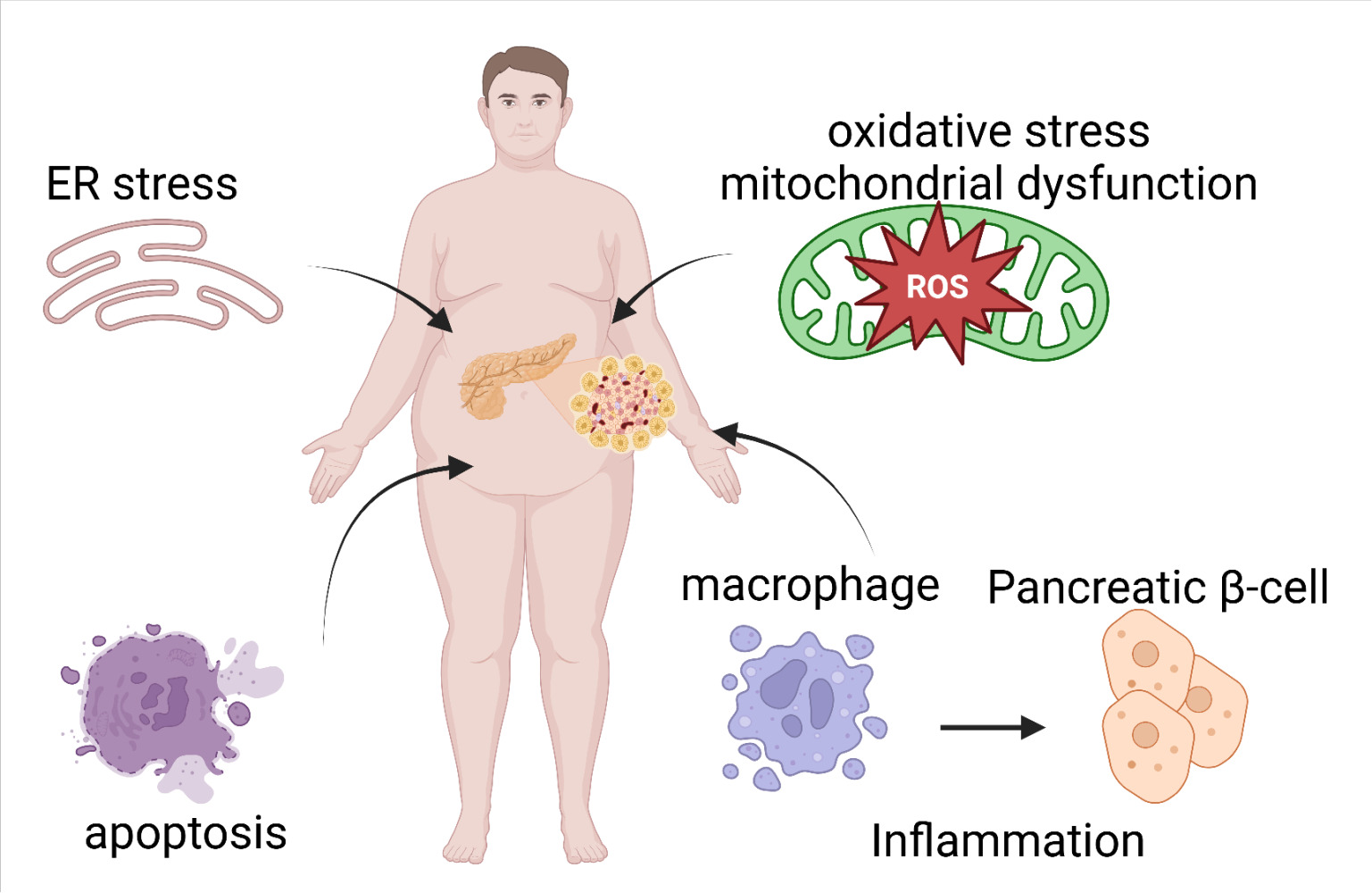
The concept of glucolipotoxicity posits a vicious cycle where elevated glucose and free fatty acid (FFA) levels synergistically impair metabolic homeostasis, a cornerstone in the pathophysiology of DKD. Lipotoxicity, the ectopic accumulation of lipids in non-adipose tissues, critically exacerbates hyperglycemia through a multi-organ mechanism, primarily by compromising pancreatic β-cell function, intensifying insulin resistance in peripheral tissues, and promoting aberrant glucose production in the liver.63
Chronic exposure to elevated FFAs, particularly saturated ones like palmitate, inflicts direct damage on pancreatic β-cells. This occurs via the induction of endoplasmic reticulum (ER) stress and mitochondrial dysfunction, which are potent triggers for cellular apoptosis. Key signaling molecules, including the transcription factors SREBP-1c and PPARs, play a complex role in this process. While PPARγ activation can be protective, its FFA-induced downregulation impairs insulin secretion.64 Furthermore, palmitate-induced ER stress activates pro-inflammatory pathways such as NF-κB and JNK, further contributing to β-cell demise.54 Evidence from in vitro studies using cell lines like INS-1E and animal models such as db/db mice confirms that lipotoxicity leads to a progressive loss of β-cell mass and function, thereby crippling the body’s ability to mount an adequate insulin response to hyperglycemia.65
Concurrently, lipotoxicity is a major driver of insulin resistance in skeletal muscle and the liver. The accumulation of lipid intermediates like diacylglycerols (DAGs) and ceramides interferes directly with the insulin signaling cascade. Recent findings from 2022–2024 confirm that in renal cells, the DAG-protein kinase C (PKC) axis is a central mechanism through which lipotoxicity induces insulin resistance.66 For instance, certain GLP-1 receptor agonists have been shown to exert protective effects by inhibiting the DAG/PKC pathway, thereby mitigating lipid-induced cellular damage.67 These kinases phosphorylate insulin receptor substrate 1 (IRS-1) on inhibitory serine residues, effectively blocking downstream signaling and blunting insulin-mediated glucose uptake.68,69
Lipotoxicity directly fuels hepatic gluconeogenesis, further worsening the hyperglycemic state. Elevated FFAs have been shown to increase the expression and activity of key gluconeogenic enzymes, namely phosphoenolpyruvate carboxykinase (PEPCK) and glucose-6-phosphatase (G6Pase).70 This is mechanistically linked to the inhibition of the Akt signaling pathway. Suppressed Akt activity allows the transcription factor FOXO1 to remain active within the nucleus, where it collaborates with coactivators like PGC-1α to drive the expression of gluconeogenic genes.71 This sustained, inappropriate production of glucose by the liver represents a critical feed-forward loop that perpetuates the hyperglycemic environment central to the initiation and progression of DKD.
Converging on Inflammation and Oxidative Stress: The Final Common Pathway
In glomerular cells (specifically podocytes), oxidative stress is a key driver of podocyte injury and albuminuria. In this compartment, the primary sources of ROS are NADPH oxidase 5 (NOX5) and mitochondrial dysfunction.55 Under hyperglycemic conditions, podocyte-specific expression of NOX5 is significantly upregulated, leading to a surge in ROS production that directly causes foot process effacement and apoptosis.56 Concurrently, high glucose impairs mitochondrial function, resulting in electron transport chain leakage and further generation of mitochondrial ROS, which creates a vicious cycle of oxidative damage and energy deficit, ultimately culminating in podocyte loss72 (Table 3).
 |
Table 3 Key Pro-Inflammatory and Profibrotic Cytokines in DKD |
In tubular epithelial cells, in contrast, the oxidative stress landscape is predominantly governed by NADPH oxidase 4 (NOX4).55 Sustained hyperglycemia and lipid overload stimulate NOX4 activity, which is a major contributor to the generation of hydrogen peroxide. This ROS production drives tubular interstitial fibrosis and inflammation, key features of progressive DKD.57,74 However, the role of NOX4 can be complex, as some studies suggest it may have context-dependent protective effects. Nevertheless, the evidence strongly supports that tubular oxidative stress, largely driven by NOX4, contributes independently to renal decline, a concept reinforced by the pathology of nonalbuminuric DKD, which often presents with severe tubulointerstitial lesions despite minimal glomerular changes.75
In parallel, glucolipotoxicity activates multiple inflammatory cascades. This is prominently observed through the activation of the NLRP3 inflammasome, a multiprotein complex that, when triggered by metabolic stress signals like ROS, cleaves pro-caspase-1 to its active form. Activated caspase-1 then facilitates the maturation and secretion of potent pro-inflammatory cytokines, including Interleukin-1β (IL-1β) and Interleukin-18 (IL-18).53 These, along with other critical mediators like Tumor Necrosis Factor-α (TNF-α) and Monocyte Chemoattractant Protein-1 (MCP-1), perpetuate a state of chronic, low-grade inflammation that recruits immune cells and directly injures renal tissue (Table 1).73,76 This inflammatory milieu is a potent activator of the master profibrotic cytokine, transforming growth factor-beta 1 (TGF-β1).58,59 Activated TGF-β1 signaling then orchestrates the excessive deposition of extracellular matrix, leading to glomerulosclerosis and tubulointerstitial fibrosis—the ultimate hallmarks of end-stage DKD.40
Therapeutic Implications
The recognition of glucolipotoxicity as a central pathogenic mechanism in DKD has prompted a fundamental evolution in therapeutic strategies. The clinical focus has broadened beyond singular glycemic control to encompass multi-target interventions aimed at the core metabolic dysregulation. This section reviews established and emerging therapies that modulate the pathological crosstalk between glucose and lipid metabolism, with the objective of preserving renal function (Table 4).
 |
Table 4 Therapeutic Strategies Targeting Glucolipid Metabolic Crosstalk in DKD |
Current Therapies Targeting Metabolic Crosstalk
Recent breakthroughs in DKD management have been led by two classes of drugs, Sodium-Glucose Cotransporter-2 inhibitors (SGLT2i) and Glucagon-Like Peptide-1 Receptor Agonists (GLP-1RAs), which have demonstrated profound renoprotective effects extending beyond their glucose-lowering capabilities. Their success lies in their ability to address the intertwined nature of glucolipid metabolism.
SGLT2 Inhibitors
SGLT2 inhibitors, such as dapagliflozin, canagliflozin, and empagliflozin, primarily act by promoting urinary glucose excretion. However, their benefits in DKD are multifactorial. By reducing plasma glucose, they alleviate glucotoxicity. Large-scale clinical trials, including the CREDENCE, DAPA-CKD, and EMPA-KIDNEY studies, have consistently shown that SGLT2i significantly reduce the risk of DKD progression.77,78 Mechanistically, this glucosuria induces a mild, persistent state of ketosis, indicating a systemic metabolic shift towards FAO and away from glycolysis for energy production. This is particularly beneficial for the kidney, as it helps restore the preferred metabolic substrate for tubular cells and reduces the burden of intracellular lipid accumulation.79 In animal models of DKD, SGLT2i have been shown to ameliorate renal steatosis, suppress oxidative stress, and reduce inflammation, effects directly linked to the correction of metabolic inflexibility.80
GLP-1 Receptor Agonists
GLP-1RAs, such as semaglutide and liraglutide, have also demonstrated significant kidney benefits. The recently concluded FLOW trial provided definitive evidence, showing that semaglutide reduced the risk of a composite primary kidney endpoint by 24% in patients with type 2 diabetes and CKD.81 Beyond improving insulin sensitivity and glucose control, GLP-1RAs exert direct effects on lipid metabolism and inflammation. They have been shown to reduce visceral adipose tissue, decrease circulating levels of triglycerides, and directly suppress inflammatory pathways like NF-κB within renal cells.82 Studies in db/db mice have shown that GLP-1RA treatment can reverse renal lipid accumulation by promoting FAO through the activation of AMP-activated protein kinase (AMPK), a master regulator of cellular energy homeostasis.83
Emerging Therapeutic Targets
Building on the success of SGLT2i and GLP-1RAs, research is now focused on more specific molecular targets at the heart of the glucolipotoxic vicious cycle.
Targeting Fatty Acid Oxidation (PPARα)
As impaired FAO is a key driver of tubular injury, agents that can restore this pathway are of great interest. Peroxisome proliferator-activated receptor alpha (PPARα) agonists, such as fenofibrate, have been investigated for this purpose. While clinical results on hard renal outcomes have been mixed, fenofibrate has been shown to slow the progression of albuminuria, and mechanistic studies confirm it can upregulate key FAO enzymes in the kidney.84 Novel, more specific FAO activators are in preclinical development, aiming to restore tubular metabolic function without the systemic side effects of older pan-PPAR agonists.
Targeting NLRP3 Inflammasome
Targeting the final common pathways of inflammation, particularly the NLRP3 inflammasome, represents another key strategy. Several small molecule NLRP3 inhibitors are now in development. While preclinical studies using various compounds have shown protection in mouse models of DKD by blocking IL-1β and IL-18 release, clinical translation is emerging.53,88 A recent Phase II trial (DAPAN-DIA) is investigating the oral selective inhibitor Dapansutrile (OLT1177) in patients with type 2 diabetes, although its primary endpoints focus on glycemic control rather than renal function.85,86 More promising for direct renal application are novel preclinical candidates, such as the highly selective “compound 32”. A 2023 study demonstrated that this molecule, possessing a novel oxazole scaffold, robustly suppressed inflammasome activity and, most notably, dose-dependently and significantly reduced the urinary albumin-to-creatinine ratio (UACR) in a mouse model of glomerulonephritis, showcasing its strong potential for treating kidney disease.87
Targeting the TXNIP-mTOR-Autophagy Axis
Finally, the TXNIP-mTOR-autophagy axis represents a novel and compelling therapeutic target. Given that hyperglycemia upregulates the pro-inflammatory protein TXNIP, which in turn activates the mTOR complex and suppresses protective autophagy, agents that can break this link are highly sought after. Metformin is known to activate autophagy via AMPK, but more specific autophagy inducers are being explored. A recent study demonstrated that silencing TXNIP restored autophagic flux and protected human kidney tubular cells from high glucose-induced apoptosis.52 Pharmacological inhibition of TXNIP or direct activation of autophagy could therefore be a powerful strategy to enhance the clearance of damaged organelles and toxic lipid species, directly counteracting the cellular damage in DKD.
Conclusion and Future Perspectives
The understanding of DKD pathogenesis has fundamentally shifted from a glucocentric view to a model driven by the synergistic toxicity of glucose and lipids. As detailed in this review, these metabolic disturbances do not operate in isolation; rather, they engage in a deleterious crosstalk where glucotoxicity fuels renal lipid accumulation, and lipotoxicity reciprocally impairs insulin signaling and mitochondrial function. This metabolic “vicious cycle” creates a self-perpetuating engine of cellular stress, ultimately converging on inflammation and fibrosis. The profound clinical efficacy of metabolic modulators, such as SGLT2 inhibitors and GLP-1 receptor agonists, serves as robust validation for this integrated metabolic perspective.
Looking forward, the therapeutic landscape must evolve from broad metabolic control to precision targeting of specific molecular nodes. Rigorous investigation is warranted for agents that directly restore renal energetics, such as selective PPARα agonists or PGC-1α activators, to reverse the core defect of FAO. Similarly, breaking the inflammatory link through novel small-molecule NLRP3 inhibitors, or restoring cellular clearance via modulation of the TXNIP-mTOR autophagy axis, represents high-value avenues for halting disease progression.
Crucially, the translation of these mechanisms into clinical practice requires the adoption of omics-based stratification. By integrating metabolomics and transcriptomics, future diagnostic frameworks could phenotype patients based on their dominant driver—whether mitochondrial dysfunction, lipotoxicity, or inflammation—facilitating the deployment of highly targeted combinatorial therapies. For the practicing clinician, this underscores a practical imperative: effective DKD management is no longer just about lowering HbA1c, but demands a holistic strategy that aggressively targets both glucose and lipid abnormalities to break the metabolic vicious cycle and preserve long-term renal function.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Author Contributions
Junying Cao: Conceptualization, Writing – original draft, Writing – review & editing. Zhihua Dun: Data curation, Writing – review & editing. Dandan Tian: Data curation, Writing – review & editing. Zhihui Qiao: Writing – review & editing, Visualization. Yuehua Wang: Conceptualization, Supervision, Project administration, Writing – review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Science Foundation of Hebei Province [Grant Number H2025423211].
Disclosure
The authors declare that they have no competing interests.
References
1. Kovesdy CP. Epidemiology of chronic kidney disease: an update 2022. Kidney Int Suppl. 2022;12(1):7–16. doi:10.1016/j.kisu.2021.11.003
2. Rafferty Q, Stafford LK, Vos T, et al. Global, regional, and national prevalence of kidney failure with replacement therapy and associated aetiologies, 1990–2023: a systematic analysis for the Global Burden of Disease Study 2023. Lancet Glob Health. 2025;13(8):e1378–e1395. doi:10.1016/S2214-109X(25)00198-6
3. Mark PB, Stafford LK, Grams ME, et al. Global, regional, and national burden of chronic kidney disease in adults, 1990–2023, and its attributable risk factors: a systematic analysis for the Global Burden of Disease Study 2023. Lancet. 2025;406(10518):2461–2482. doi:10.1016/S0140-6736(25)01853-7
4. Ma X, Liu R, Xi X, et al. Global burden of chronic kidney disease due to diabetes mellitus, 1990–2021, and projections to 2050. Front Endocrinol. 2025;16:1513008. doi:10.3389/fendo.2025.1513008
5. Deng Y, Li N, Wu Y, et al. Global, regional, and national burden of diabetes-related chronic kidney disease from 1990 to 2019. Front Endocrinol. 2021;12:672350. doi:10.3389/fendo.2021.672350
6. de Boer IH, Rue T, Hall YN, et al. Temporal trends in the prevalence of diabetic kidney disease in the United States. JAMA. 2011;305(24):2532–2539. doi:10.1001/jama.2011.861
7. Han Y-Z, Du B-X, Zhu X-Y, et al. Lipid metabolism disorder in diabetic kidney disease. Front Endocrinol. 2024;15:1336402. doi:10.3389/fendo.2024.1336402
8. Mitrofanova A, Merscher S, Fornoni A. Kidney lipid dysmetabolism and lipid droplet accumulation in chronic kidney disease. Nat Rev Nephrol. 2023;19(10):629–645. doi:10.1038/s41581-023-00741-w
9. Rayego-Mateos S, Morgado-Pascual JL, Opazo-Ríos L, et al. Pathogenic pathways and therapeutic approaches targeting inflammation in diabetic nephropathy. Int J Mol Sci. 2020;21(11):3798. doi:10.3390/ijms21113798
10. Vallon V, Thomson SC. The tubular hypothesis of nephron filtration and diabetic kidney disease. Nat Rev Nephrol. 2020;16(5):317–336. doi:10.1038/s41581-020-0256-y
11. Zhang Y, Ma KL, Liu J, et al. Dysregulation of low-density lipoprotein receptor contributes to podocyte injuries in diabetic nephropathy. Am J Physiol Endocrinol Metab. 2015;308(6):E486–E498. doi:10.1152/ajpendo.00591.2014
12. Liu X, Zhang C, Fu Y, et al. Inflammation, apoptosis, and fibrosis in diabetic nephropathy: molecular crosstalk in proximal tubular epithelial cells and therapeutic implications. Curr Issues Mol Biol. 2025;47(11):885. doi:10.3390/cimb47110885
13. Yu W, Haoyu Y, Ling Z, et al. Targeting lipid metabolic reprogramming to alleviate diabetic kidney disease: molecular insights and therapeutic strategies. Front Immunol. 2025;16:1549484. doi:10.3389/fimmu.2025.1549484
14. Rico-Fontalvo J, Aroca G, Cabrales J, et al. Molecular mechanisms of diabetic kidney disease. Int J Mol Sci. 2022;23(15):8668. doi:10.3390/ijms23158668
15. Mima A, Nomura A, Yasuzawa T. Update on the pathophysiology and treatment of diabetic kidney disease: a narrative review. Expert Rev Clin Immunol. 2025;21(9):921–928. doi:10.1080/1744666X.2025.2521086
16. Joumaa JP, Raffoul A, Sarkis C, et al. Mechanisms, biomarkers, and treatment approaches for diabetic kidney disease: current insights and future perspectives. J Clin Med. 2025;14(3):727. doi:10.3390/jcm14030727
17. Mitrofanova A, Sosa MA, Fornoni A. Lipid mediators of insulin signaling in diabetic kidney disease. Am J Physiol Renal Physiol. 2019;317(5):F1241–F1252. doi:10.1152/ajprenal.00379.2019
18. Hughes E, Wang XX, Sabol L, et al. Role of nuclear receptors, lipid metabolism, and mitochondrial function in the pathogenesis of diabetic kidney disease. Am J Physiol Renal Physiol. 2025;329(2):F225–F239. doi:10.1152/ajprenal.00110.2025
19. Alicic RZ, Rooney MT, Tuttle KR. Diabetic kidney disease: challenges, progress, and possibilities. Clin J Am Soc Nephrol. 2017;12(12):2032–2045. doi:10.2215/CJN.11491116
20. Fioretto P, Mauer M. The Jigsaw Puzzle of diabetic nephropathy. Diabetes. 2018;67(5):799–801. doi:10.2337/dbi18-0005
21. Reidy K, Kang HM, Hostetter T, Susztak K. Molecular mechanisms of diabetic kidney disease. J Clin Invest. 2014;124(6):2333–2340. doi:10.1172/JCI72271
22. Forbes JM, Cooper ME. Mechanisms of diabetic complications. Physiol Rev. 2013;93(1):137–188. doi:10.1152/physrev.00045.2011
23. Bairiskelienė I, Balion Z, Žlibinaitė L. Advanced glycation end products and their impact on diabetic kidney disease: a literature review. Nutrients. 2025;17(5):758. doi:10.3390/nu17050758
24. Zhou Y, Wang Y, Zhang T, Chen S. RAGE as a multifaceted therapeutic target in chronic kidney disease. Int J Mol Sci. 2024;25(6):3086. doi:10.3390/ijms25063086
25. Eleftheriadis T, Pissas G, Antoniadi G, Liakopoulos V. Targeting the RAGE-DIAPH1-oxidative stress axis in diabetic nephropathy. Rom J Diabetes Nutr Metabol Dis. 2024;31(2):123–131. doi:10.47803/rjdnd.2024.31.2.123
26. Gabbay KH, Balko C, Gabbay KH. The sorbitol pathway and the complications of diabetes. N Engl J Med. 1973;288(16):831–836. doi:10.1056/NEJM197304192881609
27. Fuhr L, Vasconcellos LR, Marques F, et al. Hyperglycemia in diabetes: beyond the polyol pathway. Biomed Pharmacother. 2022;153:113425. doi:10.1016/j.biopha.2022.113425
28. Li Q, Li H, Chen Z, et al. Aldose reductase: a key player in the pathophysiology of diabetic complications and a hope for the future. Biomolecules. 2021;11(5):730. doi:10.3390/biom11050730
29. Welsh GI, Hale LJ, Eremina V, et al. Insulin signaling to the glomerular podocyte is critical for normal kidney function. Cell Metab. 2010;12(4):329–340. doi:10.1016/j.cmet.2010.08.014
30. Artunc F, Schleicher E, Weigert C, Fritsche A, Stefan N, Häring H-U. The impact of insulin resistance on the kidney and vasculature. Nat Rev Nephrol. 2016;12(12):721–737. doi:10.1038/nrneph.2016.145
31. Kang HM, Ahn SH, Choi P, et al. Defective fatty acid oxidation in renal tubular epithelial cells has a key role in kidney fibrosis development. Nat Med. 2015;21(1):37–46. doi:10.1038/nm.3762
32. Hall AM, Lale-Farjat SL, Farsijani NM, et al. Mitochondrial dysfunction in kidney disease. Nat Rev Nephrol. 2018;14(5):291–311. doi:10.1038/nrneph.2018.9
33. Sun M, Liu Z, Zhou S, et al. Targeting mitochondrial dysfunction: a potential therapeutic strategy for diabetic kidney disease. Cell Mol Life Sci. 2024;81(1):52. doi:10.1007/s00018-023-05078-y
34. Stanigut AM, Pana C, Enciu M, Deacu M, Stancu S, Iorga R. Hypoxia-inducible factors and diabetic kidney disease—how deep can we go? Int J Mol Sci. 2022;23(18):10413. doi:10.3390/ijms231810413
35. Park J, Joo YS, Nam BY, et al. Pyruvate kinase M2 activation maintains mitochondrial metabolism by regulating the interaction between HIF-1α and PGC-1α in diabetic kidney disease. Mol Med. 2025;31(1):161. doi:10.1186/s10020-025-01320-4
36. Herman-Edelstein M, Scherzer P, Tobar A, et al. Altered renal lipid metabolism and renal lipid accumulation in human diabetic nephropathy. J Lipid Res. 2014;55(3):561–572. doi:10.1194/jlr.P040502
37. Sun Y, Cui S, Hou Y, Yi F. The updates of podocyte lipid metabolism in proteinuric kidney disease. Kidney Dis. 2021;7(6):438–451. doi:10.1159/000518132
38. Feng A, Yin R, Xu R, Zhang B, Yang L. An update on renal tubular injury as related to glycolipid metabolism in diabetic kidney disease. Front Pharmacol. 2025;16:1559026. doi:10.3389/fphar.2025.1559026
39. Wang Y, Li Y, Ma Z, et al. PPARα in diabetic kidney disease: biological function and therapeutic potential. Front Endocrinol. 2023;14:1120092. doi:10.3389/fendo.2023.1120092
40. Ma X, Ma J, Leng T, et al. Advances in oxidative stress in pathogenesis of diabetic kidney disease and efficacy of TCM intervention. Ren Fail. 2023;45(1):2146512. doi:10.1080/0886022X.2022.2146512
41. Hua Y, Zhang Z, Li X, et al. Single-cell and spatial transcriptomics reveal lipid metabolism dysregulation in human diabetic kidney disease. Nat Commun. 2023;14(1):5822. doi:10.1038/s41467-023-41589-3
42. Laplante M, Sabatini DM. mTORC1 activates SREBP-1c and uncouples lipogenesis from gluconeogenesis. Proc Natl Acad Sci U S A. 2010;107(8):3281–3282. doi:10.1073/pnas.1000323107
43. Godel M, Hartleben B, Herbach N, et al. mTORC1 activation in podocytes is a critical step in the development of diabetic nephropathy in mice. Cell Metab. 2011;13(6):627–638. doi:10.1016/j.cmet.2011.03.020
44. Wu M, Yang Z, Zhang C, et al. Inhibition of NLRP3 inflammasome ameliorates podocyte damage by suppressing lipid accumulation in diabetic nephropathy. Metabolism. 2021;116:154460. doi:10.1016/j.metabol.2021.01.002
45. Liu P, Zhang Z, Li Y. Relevance of the pyroptosis-related inflammasome pathway in the pathogenesis of diabetic kidney disease. Front Immunol. 2021;12:603416. doi:10.3389/fimmu.2021.603416
46. Jia G, Wharram B, Shilesh C, et al. The interaction of fatty acids and AMP-activated protein kinase in the pathogenesis of diabetic nephropathy. Diabetes. 2009;58(5):1046–1058. doi:10.2337/db08-1002
47. Opazo-Ríos L, Mas S, Marín-Royo G, et al. Lipotoxicity and diabetic kidney disease: a dangerous liaison. Biomedicines. 2020;8(10):436. doi:10.3390/biomedicines8100436
48. Herman MA, Peroni OD, Villoria J, et al. A novel ChREBP isoform in adipose tissue regulates systemic glucose metabolism. Nature. 2012;484(7394):333–338. doi:10.1038/nature10986
49. Du Y, Li R, Liu T, et al. Hyperglycemia-driven renal lipid accumulation is mediated by the ChREBP/miR-33a-5p axis. JCI Insight. 2022;7(13):e155822. doi:10.1172/jci.insight.155822
50. Zhu Q, Wu X, Di Y, Liu L, Liu Y. The TXNIP–mTOR–Autophagy axis in diabetic kidney disease: mechanistic insights and therapeutic implications. Mol Biol Rep. 2025;52(1):839. doi:10.1007/s11033-025-10946-w
51. Sun H, Sun R, Hua Y, Lu Q, Shao X. An update on the role of thioredoxin-interacting protein in diabetic kidney disease: a mini review. Front Med. 2023;10:1153805. doi:10.3389/fmed.2023.1153805
52. Du Y, Wu M, Song S, Bian Y, Shi Y. TXNIP deficiency attenuates renal fibrosis by modulating mTORC1/TFEB-mediated autophagy in diabetic kidney disease. Ren Fail. 2024;46(1):2338933. doi:10.1080/0886022X.2024.2338933
53. Luo Y, Long M, Wu X, Zeng L. Targeting the NLRP3 inflammasome in kidney disease: molecular mechanisms, pathogenic roles, and emerging small-molecule therapeutics. Front Immunol. 2025;16:1703560. doi:10.3389/fimmu.2025.1703560
54. Gorasia DG, Dud-Bbusamsub MS, Dholariya SJ, et al. The role of oxidative stress in pancreatic β cell dysfunction in diabetes. Int J Mol Sci. 2021;22(4):1509. doi:10.3390/ijms22041509
55. Wang N, Zhang C. Oxidative stress: a culprit in the progression of diabetic kidney disease. Antioxidants. 2024;13(4):455. doi:10.3390/ant13040455
56. Jha JC, Dai A, Garzarella J, et al. Independent of renox, NOX5 promotes renal inflammation and fibrosis in diabetes by activating ROS-sensitive pathways. Diabetes. 2022;71(6):1282–1297. doi:10.2377/db21-0941
57. Vodošek Hojs N, Bevc S, Ekart R, et al. Oxidative stress markers in chronic kidney disease with emphasis on diabetic nephropathy. Antioxidants. 2020;9(10):925. doi:10.3390/antiox9100925
58. Sanchez-Niño MD, Benito-Martin A, Ortiz A. Key profibrotic and pro-inflammatory pathways in the pathogenesis of diabetic kidney disease. Diab Vasc Dis Res. 2021;18(3):147916412110250. doi:10.1177/14791641211025032
59. Ricardo-Lax I, Holland C, MacPhee I, et al. Kidney fibrosis and oxidative stress: from molecular pathways to new pharmacological opportunities. Biomolecules. 2024;14(1):137. doi:10.3390/biom14010137
60. Chen J, Chen JK, Harris RC. The role of renal insulin resistance in the pathogenesis of diabetic kidney disease. Front Med. 2022;9:835928. doi:10.3389/fmed.2022.835928
61. Zhou Z, Li M, Zhang Y, et al. The crosstalk between insulin resistance and kidney diseases. Front Endocrinol. 2023;14:1169999. doi:10.3389/fendo.2023.1169999
62. Chen J, Gu S, Chen J, et al. Thioredoxin-interacting protein (TXNIP) in chronic kidney disease. Clin Chim Acta. 2025;581:118123. doi:10.1016/j.cca.2025.118123
63. Opazo-Ríos L, Mas S, Marín-Royo G, et al. Lipotoxicity and diabetic nephropathy: novel mechanistic insights and therapeutic opportunities. Int J Mol Sci. 2020;21(7):2632. doi:10.3390/ijms21072632
64. Schultheis J, Beckmann D, Mulac D, Müller L, Esselen M, Düfer M. Nrf2 activation protects mouse beta cells from glucolipotoxicity by restoring mitochondrial function and physiological redox balance. Oxid Med Cell Longev. 2019;2019:7518510. doi:10.1155/2019/7518510
65. Cnop M, Abdul-Ghani MA, DeFronzo RA, Igoillo-Esteve M. Pancreatic beta-cell dysfunction in type 2 diabetes. Sage J. 2023;5(1). doi:10.1177/1721727X231154152
66. Yazıcı D, Demir SÇ, Sezer H. Insulin resistance, obesity, and lipotoxicity. In: Obesity and Lipotoxicity. Springer; 2024:391–430. doi:10.1007/978-3-031-63657-8_14
67. Fu WJ, Huo J-L, Mao Z-H, et al. Emerging role of antidiabetic drugs in cardiorenal protection. Front Pharmacol. 2024;15. doi:10.3389/fphar.2024.1349069
68. Summers SA, Higashihara T, Inagi R. Lipotoxicity in kidney, heart, and skeletal muscle dysfunction. Nutrients. 2019;11(7):1664. doi:10.3390/nu11071664
69. Petersen MC, Shulman GI, Van Den Bosch B, Moro C. Novel insights and mechanisms of lipotoxicity-driven insulin resistance. Int J Mol Sci. 2020;21(17):6358. doi:10.3390/ijms21176358
70. Choi HE, Kim Y, Lee HJ, Cheon HG. Novel FoxO1 inhibitor, JY-2, ameliorates palmitic acid-induced lipotoxicity and gluconeogenesis in a murine model. Eur J Pharmacol. 2021;899:174011. doi:10.1016/j.ejphar.2021.174011
71. Gu H, Chen F, Zhang Q, et al. Spexin alleviates insulin resistance and inhibits hepatic gluconeogenesis via the FoxO1/PGC-1α pathway in high-fat-diet-induced rats and insulin resistant cells. J Transl Med. 2019;17(1):387. doi:10.1186/s12967-019-02137-0
72. Zhu YT, Wan C, Lin J-H, et al. Mitochondrial oxidative stress and cell death in podocytopathies. Biomolecules. 2022;12(3):403. doi:10.3390/biom12030403
73. Gao P, Zhou Y, Yang S. The role of MCP-1/CCR2 signaling in diabetic kidney disease. Arch Physiol Biochem. 2022;128(5):1199–1206. doi:10.1080/13813455.2020.1762664
74. Winiarska A, Knysak K, Nabrdalik K, et al. Inflammation and oxidative stress in diabetic kidney disease: the targets for SGLT2 Inhibitors and GLP-1 receptor agonists. Int J Mol Sci. 2021;22(19):10822. doi:10.3390/ijms221910822
75. Shi S, Ni L, Gao L, et al. Comparison of nonalbuminuric and albuminuric diabetic kidney disease among patients with type 2 diabetes: a systematic review and meta-analysis. Front Endocrinol. 2022;13:871272. doi:10.3389/fendo.2022.871272
76. Tang SCW, Yiu WH. Innate immunity in diabetic kidney disease. Nat Rev Nephrol. 2020;16(4):206–222. doi:10.1038/s41581-019-0234-4
77. Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–2306. doi:10.1056/NEJMoa1811744
78. Uster A, Desai N, Navaneethan SD, Pfarr E, Mazo AR. Empagliflozin reduces risk of hospitalization in patients with chronic kidney disease in the EMPA-KIDNEY trial. Clin Ther. 2025;47(12):1091–1096. doi:10.1016/j.clinthera.2025.09.005
79. Sano M. A new class of drugs for heart failure: SGLT2 inhibitors reduce sympathetic overactivity. J Cardiol. 2018;71(5):471–476. doi:10.1016/j.jjcc.2017.12.004
80. Kawanami D, Matoba K, Takeda Y, et al. SGLT2 inhibitors as a therapeutic option for diabetic kidney disease. Int J Mol Sci. 2021;22(20):11255. doi:10.3390/ijms222011255
81. Groop PH, Ji L, Rossing P, et al. Semaglutide and kidney outcomes in type 2 diabetes and chronic kidney disease. N Engl J Med. 2024;391(2):109–121. doi:10.1056/NEJMoa2403347
82. Mann JFE, Ørsted DD, Brown-Frandsen K, et al. Liraglutide and renal outcomes in type 2 diabetes. N Engl J Med. 2017;377(9):839–848. doi:10.1056/NEJMoa1616011
83. Tian S, Zhou S, Wu W, et al. GLP-1 receptor agonists alleviate diabetic kidney injury via β-klotho-mediated ferroptosis inhibition. Adv Sci. 2025;12(4):e2409781. doi:10.1002/advs.202409781
84. Davis TM, Ting R, Best JD, et al. Effects of fenofibrate on renal function in patients with type 2 diabetes mellitus: the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) Study. Diabetologia. 2011;54(2):280–290. doi:10.1007/s00125-010-1951-1
85. Fang B, Huang W, Du S, et al. The inflammatory cell death in diabetic kidney disease: integrating multifactorial mechanisms into novel therapeutics. Int J Mol Sci. 2025;26(22):11033. doi:10.3390/ijms262211033
86. Hepprich M, Esser N, Julla JB, et al. NLRP3 inflammasome inhibition with dapansutrile in type 2 diabetes and elevated systemic inflammation: rationale and design of the DAPAN-DIA study. Circulation. 2024;150(Suppl_1):A4115645. doi:10.1161/circ.150.suppl_1.4115645
87. Ohba Y, Adachi K, Furukawa T, et al. Discovery of novel NLRP3 inflammasome inhibitors composed of an oxazole scaffold bearing an acylsulfamide. ACS Med Chem Lett. 2023;14(12):1833–1838. doi:10.1021/acsmedchemlett.3c00433
88. Wu M, Yang Z, Zhang C, et al. Inhibition of NLRP3 inflammasome ameliorates podocyte damage by suppressing lipid accumulation in diabetic nephropathy. Metabolism. 2021;118:154748. doi:10.1016/j.metabol.2021.154748
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Platelet-Activating Factor Promotes the Development of Non-Alcoholic Fatty Liver Disease
Yin H, Shi A, Wu J
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2003-2030
Published Date: 8 July 2022
Therapeutic Approaches for Nonalcoholic Fatty Liver Disease: Established Targets and Drugs
Huang X, Chen H, Wen S, Dong M, Zhou L, Yuan X
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1809-1819
Published Date: 21 June 2023
Correlation Between Serum Vitamin E and HOMA-IR in Patients with T2DM
Zhang J, Hou Y, Zhang Z, Shi Y, Wang Z, Song G
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1833-1843
Published Date: 23 April 2024
Lipotoxicity: A New Perspective in Type 2 Diabetes Mellitus
Chen B, Li T, Wu Y, Song L, Wang Y, Bian Y, Qiu Y, Yang Z
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1223-1237
Published Date: 24 April 2025
Glycolytic Dysfunction in Granulosa Cells and Its Contribution to Metabolic Dysfunction in Polycystic Ovary Syndrome
Cao Z, Zhou Q, An J, Guo X, Jia X, Qiu Y
Drug Design, Development and Therapy 2025, 19:5255-5270
Published Date: 18 June 2025