Back to Journals » Clinical Epidemiology » Volume 18
Positive Predictive Values of Familial Hypercholesterolemia Diagnoses in the Danish National Patient Registry and the Danish Familial Hypercholesterolemia Registry – A Validation Study
Authors Knold J ![]() , Bork C, Snoer M, Heitmann M, Bang LE, Kanstrup H, Hansen KL
, Bork C, Snoer M, Heitmann M, Bang LE, Kanstrup H, Hansen KL ![]() , Hedegaard BS, Thomsen KK, Lauridsen BK, Bovin A, Lundquist AA, Al Tamimi HKS, Brorholt-Petersen JU, Christensen TE, Bertelsen MLN, Gohr T, Ellermann A
, Hedegaard BS, Thomsen KK, Lauridsen BK, Bovin A, Lundquist AA, Al Tamimi HKS, Brorholt-Petersen JU, Christensen TE, Bertelsen MLN, Gohr T, Ellermann A ![]() , Hansen CP, Weis A, Nielsen PR, Schmidt EB, Bundgaard H, Henriksen FL
, Hansen CP, Weis A, Nielsen PR, Schmidt EB, Bundgaard H, Henriksen FL
Received 4 August 2025
Accepted for publication 21 January 2026
Published 11 February 2026 Volume 2026:18 556764
DOI https://doi.org/10.2147/CLEP.S556764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Irene Petersen
Familial Hypercholesterolemia Diagnoses in Danish Registries – Video abstract [556764]
Views: 35
Jakob Knold,1,2 Christian Bork,3,4 Martin Snoer,5 Merete Heitmann,6,7 Lia Evi Bang,8 Helle Kanstrup,9,10 Kristoffer Lund Hansen,11 Berit Storgaard Hedegaard,12 Kristian Korsgaard Thomsen,2,13 Bo Kobberø Lauridsen,14 Ann Bovin,15 Alberte Aspaas Lundquist,16 Hassan Kussai Salem Al Tamimi,17 Jens Uffe Brorholt-Petersen,18 Thomas Emil Christensen,19 Mette Lykke Norgaard Bertelsen,20 Thomas Gohr,21 Annie Ellermann,22 Camilla Plambeck Hansen,23 Anette Weis,23 Philip Rising Nielsen,23 Erik Berg Schmidt,3,4 Henning Bundgaard,7,8 Finn Lund Henriksen1,2 On behalf of the Danish Familial Hypercholesterolemia Study Group
1Department of Cardiology, Odense University Hospital, Odense, Denmark; 2Clinical Institute, University of Southern Denmark, Odense, Denmark; 3Department of Cardiology, Aalborg University Hospital, Aalborg, Denmark; 4Department of Clinical Medicine, Aalborg University, Aalborg, Denmark; 5Department of Cardiology, Zeeland University Hospital, Roskilde, Denmark; 6Department of Cardiology, University Hospital Bispebjerg-Frederiksberg, Copenhagen, Denmark; 7Institute for Clinical Medicine, University of Copenhagen, Copenhagen, Denmark; 8Department of Cardiology, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark; 9Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark; 10Department of Clinical Medicine, Aarhus University, Aarhus, Denmark; 11Department of Cardiology, Hospital of Southern Jutland, Aabenraa, Denmark; 12Department of Cardiology, Viborg-Silkeborg-Skive Regional Hospital, Viborg, Denmark; 13Department of Cardiology, Hospital of Southwest Jutland, Esbjerg, Denmark; 14Department of Cardiology, Herlev-Gentofte Hospital, Copenhagen, Denmark; 15Department of Cardiology, Hospital of Lille Baelt, Vejle, Denmark; 16Department of Paediatrics and Adolescent Medicine, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark; 17Department of Cardiology, Naestved, Slagelse, Ringsted Hospital, Slagelse, Denmark; 18Department of Cardiology, Goedstrup Hospital, Goedstrup, Denmark; 19Department of Cardiology, Amager-Hvidovre Hospital, Copenhagen, Denmark; 20Department of Cardiology, North Zeeland University Hospital, Hilleroed, Denmark; 21Department of Cardiology, Lille Baelt Hospital, Kolding, Denmark; 22Department of Pediatrics, Holbaek Hospital, Holbaek, Denmark; 23The Danish Healthcare Quality Institute, Aalborg, Denmark
Correspondence: Jakob Knold, Email [email protected]
Introduction: The Danish Familial Hypercholesterolemia (FH) Registry (DFH) was established in 2020 to monitor the detection rate of FH and quality of care provided among patients with FH. DFH is nationwide, and together with the Danish National Patient Registry (DNPR) includes more than 10,000 registered cases of FH. However, the validity of FH diagnoses in the DNPR and DFH is unknown.
Purpose: We aimed to investigate the positive predictive value of FH cases registered in the DNPR and DFH.
Methods: We retrospectively retrieved a nationwide random sample of 800 patients with an FH diagnosis registered in the DNPR between 1st of January 2020 and 1st of May 2023. Subsequently, we retrieved information on cases also registered in the DFH, and validated all registered cases based on medical records. Individuals with a Dutch Lipid Clinical Network-score ≥ 6 were considered valid FH cases. Positive predictive values with 95% confidence intervals were used to assess the validity of the registered diagnoses.
Results: We found a positive predictive value of 63.8% (95% CI: 60.7; 67.0) for an FH diagnosis recorded in the DNPR (510/800), and 88.1% (95% CI: 82.2; 92.3%) for those diagnosed with genetic FH (141/160). A primary diagnosis of FH registered by cardiological departments had a positive predictive value of 71.0% (95% CI: 67.2; 74.6%) (417/587), and 88.3% (95% CI: 82.6; 92.8%) for genetic FH (113/128), respectively. The positive predictive value of FH cases registered in the DFH was 83.0% (95% CI: 78.9; 86.5) (318/383).
Conclusion: The validity of FH cases in the DFH was high, while the validity of an FH diagnosis in the DNPR was relatively low. However, restricting the analysis to a primary diagnosis obtained from cardiological departments may be used to improve the validity of FH diagnoses in the DNPR.
Keywords: validity, epidemiology, lipidology, familial hypercholesterolemia
Introduction
Familial hypercholesterolemia (FH) is a genetic disorder characterized by elevated low-density lipoprotein cholesterol (LDL-C) since birth leading to significantly increased risk of premature atherosclerotic cardiovascular disease (ASCVD) and mortality.1,2 FH is underdiagnosed and undertreated in most countries worldwide.1,3–5 Patients with heterozygote FH not receiving lipid-lowering treatment have a 15–20-fold higher risk of coronary artery disease (CAD) – particularly myocardial infarction – compared to the general population.6 Early studies conducted before the statin era reported that 25% with FH had developed CAD at age 40 increasing to 60% to 85% at age 60.7,8 In patients with homozygote FH, CAD may develop before age 12 and the median age of death is 28 years in patients not receiving advanced lipid-lowering treatment.9,10 In Denmark, detection and management of FH patients are monitored through the nationwide Danish National Patient Registry (DNPR) and the Danish Familial Hypercholesterolemia Registry (DFH).11–13 By July 2024, these registries included more than 10,000 registered cases of FH, but the validity of the diagnoses remains unknown.12,13 The prevalence of heterozygous FH in Denmark was estimated to 1 in 220 individuals corresponding to an expected Danish FH population of 27.000 individuals.14
The healthcare system in Denmark is based on a tax-funded system with free access to public hospitals and general practitioners including evaluation for FH in one of the 15 Danish lipid clinics that performs diagnostic assessment for FH.15 A total of 1,425 individuals were referred for diagnostic evaluation between 1st of July 2022 and 30th of June 2023 to one of the 15 Danish Lipid Clinics on suspicion of FH.16
The DNPR was established in 1977 and includes information on all hospital admissions, outpatient visits and treatments provided in Denmark, providing a comprehensive data source for disease identification and enabling the study of long-term temporal trends in hospitalization and treatment rates.11 The DNPR contains detailed administrative data and diagnoses classified according to the ICD-8 (International Classification of Disease, eighth revision) until the end of 1993, and ICD-10 (International Classification of Disease, tenth revision) from 1993 onwards.11 The ICD codes are registered by the discharging physician, and 99% of discharges are recorded in the DNPR.11,17 A unique personal registration number assigned to every Danish citizen at birth or upon immigration enables record linkage with other Danish registries.11
In 2020, the Danish government funded the establishment of the nationwide DFH to monitor and assess diagnostics, detection, and quality of health care provided patients with FH based upon predefined quality indicators.12,13 The objective was to improve the detection rate of patients with FH and identify areas of improvement in the management of patients with FH. The DFH includes detailed information on plasma lipid levels, including lipoprotein(a), lipid lowering treatment, genetic tests, and dietary counseling.13 The registry data combines manual entries with record linkage to Danish nationwide health registries.13 The DNPR and DFH are used for decision-making to improve FH management and utilization of healthcare resources and are anticipated to become a valuable source for research. Unfortunately, the validity of registered FH cases in the DNPR and DFH remains unknown.
We aimed to assess the positive predictive value (PPV) of registered FH cases in a random sample from both the DNPR and the DFH using information related to the Dutch Lipid Clinical Network (DLCN) score from medical records as reference.1,2 Furthermore, we aimed to develop algorithms to enhance the validity of FH case definitions and to evaluate the validity of the DLCN components in the DFH as well as the quality of selected DFH indicators.
Materials and Methods
Study Population and Design
This retrospective validation study was based on a nationwide randomly selected sample of 800 FH diagnoses registered in the DNPR between January 1st 2020 and May 1st 2023. The sample of 800 individuals registered with an FH diagnoses was randomly drawn among all registered FH diagnoses in the DNPR within the specified time frame by the Danish Healthcare Quality Institute (DHQI). Simple random sampling was used as the sample selection method. In simple random sampling, each sampling unit (observation) has an equal probability of selection, and sampling is performed without replacement. Thus, the 800 individuals included in this study were completely at random selected automatically among all FH diagnoses in the DNPR. The sample size represented approximately 8% of all registered FH cases in Denmark, and this large sample allowed for detailed stratification analyses to be used for development of algorithms that could be used to improve the validity of FH case definitions.12,13 The following ICD10 diagnoses codes for FH were included: DE780B (FH), DE780B1 (heterozygous FH) and DE780B2 (homozygous FH). We also retrieved information on the number of patients registered with two consecutive FH diagnoses in the DNPR, along with the total number of patients with a heterozygous FH diagnosis in the DNPR. Subsequently, we retrieved data from the subset of patients also registered in the DFH; including data on DLCN scores, levels of plasma lipoprotein(a), and the use of lipid-lowering medication.18
Ethical Statement
The study was obtained at the Internal List of Research Projects (23/31480) and approved by the Regional Council in the Region of Southern Denmark (23/19,548). No further ethical approval was required according to Danish law.
Definitions and Validation
Potential FH cases were categorized into those registered with an FH diagnosis (DE780B, DE780B1 or DE780B2) or with a genetic FH diagnosis (DE780B1, DE780B2) in the DNPR. Potential FH cases in the DFH in this validation study were defined as individuals registered with an FH diagnosis in the DNPR and a DLCN score ≥ 6 in the DFH. FH cases in the DFH are defined as a registered diagnosis of FH in the DNPR and/or a DLCN score ≥ 6 in the DFH.
Subsequently, we categorized potential FH cases in the DFH into clinical FH and genetic FH cases. Potential clinical FH cases in the DFH were defined as a DLCN score ≥ 6 without registration of genetic test results as well as those genetically tested, but without pathogenic FH genetic variants identified. Potential cases of genetic FH in the DFH included individuals registered as carriers of a likely pathogenic; category 4 or pathogenic; category 5 FH - variant.19 Valid FH cases were defined by a DLCN score ≥ 6 according to medical records, while valid (heterozygous) genetic FH cases were defined by a genetic test showing a likely pathogenic or pathogenic FH variant in either apolipoprotein B (ApoB)-, low-density lipoprotein receptor (LDLR)- or proprotein-convertase-subtilisin/kexin-type 9 (PCSK9) gene.1,2 Valid clinical FH cases were defined by a DLCN score ≥ 6 in subjects either not genetically tested or genetically tested without a likely pathogenic or pathogenic FH variant identified. First-degree relatives to patients with clinical FH were classified according to age- and sex-specific plasma LDL-C cut-off levels suggestive of FH according to the Danish National FH guidelines.20
Medical Record Data Collection
We retrieved information from medical records using pre-specified validation sheets. The validation sheets were tested in a small-scale test in the Northern region of Denmark including 39 individuals registered with FH available in the random sample, and only minor changes were applied after the test. Data collection included; untreated levels of plasma LDL-C, plasma lipid and lipoprotein(a) levels; historical plasma LDL-C levels, use of lipid lowering-treatment at the time of diagnosis, cardiovascular risk factors, history of ASCVD (family and individual), manifestation of arcus cornealis, tendon xanthomas, xanthelasmatas, results of genetic testing, treatment and dietary counselling by a dietitian. In addition, plasma lipid levels and lipid-lowering treatment six months after the diagnosis (± 120 days) were obtained (Supplementary Table 1). Data collection was conducted in collaboration with all Danish Lipid Clinics (n = 15) and paediatric units specialised in FH (n = 2), and included 21 specialists in lipidology trained in the validation procedure, who retrieved data from the medical records of their patients. Subsequently, information from the validation sheets were registered in a REDCapTM database.21 The random sample of 800 FH diagnosis obtained from the DNPR including the subset of patients also registered in the DFH was merged with the data obtained from medical records through linkage by the unique personal registration number.11 If untreated plasma lipid levels were not available, we estimated treatment corrected plasma LDL-C values according to the average effect on LDL-C of the lipid-lowering treatment used (Supplementary Table 2).
Statistical Analysis
We assessed the validity of FH ICD-10 diagnoses using PPVs with Wilson 95% confidence intervals (CI).22 The PPV of an FH diagnosis in the DNPR was calculated as the proportion of patients with a verified FH diagnosis among all patients registered with an FH diagnosis. Thus, all verified FH patients being the numerator and all patients registered with an FH diagnosis being the denominator. Because the accuracy of registry-based diagnoses may vary across patient groups and settings, we stratified PPVs by sex, type of diagnosis, region and departments. We explored whether validity improved when patients had two consecutive FH diagnoses, and whether probands differed from first-degree relatives. Additionally, we compared the validity of clinically defined FH with genetically verified FH. The stratified analyses were used for development of algorithms for case definitions that might improve the validity.
Subsequently, we calculated the PPV within the subset of patients registered in the DFH, defined as the proportion of verified FH cases (the numerator) among all patients with a registered DLCN score ≥ 6 in the DFH (the denominator).
The overall registry coverage of the DFH was estimated by dividing the number of patients registered in the DFH with the total number of FH diagnoses in the DNPR random sample. The coverage of valid FH cases of the DFH was estimated by dividing the number of verified FH patients registered with a DLCN score ≥ 6 in the DFH (the numerator) with all verified FH diagnoses in the DNPR random sample (the denominator). The coverage of valid genetic FH was evaluated by dividing all patients with a verified pathogenic genetic variant in the DFH (the numerator), with all verified genetic FH cases identified in the DNPR random sample (the denominator).
To evaluate the accuracy of the individual components of the DLCN score in the DFH, we calculated PPVs for each component as the proportion of verified score components among all score components registered in the DFH. We calculated the completeness (sensitivity) of each DLCN component, to reflect how often true score components were recorded in the DFH. Completeness was calculated as the proportion of verified components recorded in the DFH relative to all verified components identified in medical records for patients registered in the DFH.
Finally, we assessed the quality of a subset of DFH quality indicators by reporting the proportion of fulfilled indicators based on DFH-registered information and reporting corresponding proportions derived from medical records. Analyses were stratified by FH diagnoses in the DNPR (all and verified) and by FH cases registered in the DFH (all and verified). Risk-specific LDL-C treatment targets were defined in accordance with the Danish Dyslipidemia Guidelines from the Danish Society of Cardiology, based on risk profiles documented at the date of diagnosis.23
All statistical analyses were performed using STATA BE 18.5© (StataCorp LLC, College Station, Texas, USA).
Results
We validated a total of 800 individuals (56.5% women) registered in the DNPR with a diagnosis of FH including 473 individuals also registered in the DFH, corresponding to an overall coverage of 59.1% (95% CI: 55.6; 62.5%) of the DFH (Figure 1). Median age at diagnosis was 50.5 (IQR 31; 61) years. The majority of the diagnoses were coded as a primary diagnosis of FH (81.2%), and 83.6% of all diagnoses were registered at a cardiological department. A total of 79.8% of all registered diagnoses in the DNPR were coded with the FH diagnosis (DE780B), whereas 20.2% were registered with a genetic FH diagnosis (DE780B1 or DE780B2). Characteristics of individuals also registered in DFH were comparable to individuals with an FH diagnosis in DNPR (Table 1).
 |
Figure 1 Flow diagram of the validation of FH diagnoses. aAll FH diagnoses in the DNPR as per 1st of July 2024.16 Abbreviations: DFH, Danish Familial Hypercholesterolemia Registry; DLCN, Dutch Lipid Clinical Network Score; DNPR, Danish National Patient Registry; FH, Familial Hypercholesterolemia; n, Number. |
 |
Table 1 Characteristics |
Validity of FH Diagnoses in the DNPR
We verified a total of 510 out of 800 registered FH diagnoses corresponding to a PPV of an FH diagnosis in the DNPR of 63.8% (95% CI: 60.7; 67.0%). The PPV of an FH diagnosis was higher for primary than secondary diagnoses (69.8% vs 37.3%), and higher among first-degree relatives than for individuals registered as probands (79.9% vs 56.6%). The highest PPVs were found in the North (79.5%) and Central (77.1%) regions of Denmark. The PPV was higher in individuals registered with FH diagnoses in two separate and consecutive registrations (69.9%) (Table 2). Genetic testing was performed in 640 individuals (80.0%) of all registered FH diagnoses in the DNPR and 388 (48.5%) had a likely pathogenic or pathogenic FH variant, but only 141 (36.3%) of these were registered with a first-time diagnosis of heterozygous FH. A total of 141 out of 160 registered with a first-time diagnosis of heterozygous FH were verified corresponding to a PPV in the DNPR of 88.1% (95% CI: 82.2; 92.3%) (Table 2). When the total number of all heterozygous FH diagnoses (DE780B1) was taken into account, including those registered after the initial FH diagnosis, a total of 216 patients had a heterozygous FH diagnosis corresponding to 55.6% of the patients with a likely pathogenic or pathogenic genetic FH variant.
 |
Table 2 Positive Predictive Values for FH Diagnoses Registered in the DNPR |
Validity and Coverage of an FH Diagnosis in the DFH
We verified an FH diagnosis in 318 out of 383 individuals registered with FH (DLCN ≥ 6) in the DFH equivalent to a PPV of 83.0% (95% CI: 78.9; 86.5%) (Table 3). In the DFH, a total of 166 individuals were registered as carriers of a likely pathogenic or a definite pathogenic genetic FH variant. A likely pathogenic or a definite pathogenic variant was confirmed in 158 subjects corresponding to a PPV of genetic FH cases in the DFH of 95.2% (95% CI: 90.6; 97.5%) (Table 3).
 |
Table 3 Positive Predictive Values and Coverage of FH Cases in the DFH |
The coverage of valid FH cases in the DFH (n = 318) compared with the DNPR (n = 510) was 62.4% (95% CI: 58.1; 66.4). The DFH covered 40.7% (95% CI: 35.9; 45.7) of valid genetic FH cases (Table 3).
Algorithms to Improve the Validity of FH Case Definitions
Different algorithms for improving the validity of registered FH cases in the DNPR and the DFH were specified (Table 4). The PPV of an FH diagnosis could be improved to 71.0% (95% CI: 67.2; 74.6) (417/587) by restricting cases to a primary diagnosis of FH established at a department of cardiology. The validity could be further improved to 75.0% (95% CI: 71.1; 78.5) (396/528) by restricting cases to a primary diagnosis of FH established at units that typically diagnose patients with FH (Departments of Cardiology, Paediatrics, and Clinical Genetics) and the presence of at least two registered FH diagnoses. The number of registered genetic FH diagnoses in the DNPR did not differ appreciably according to more strict case definitions.
 |
Table 4 Algorithms for FH Case Definitions in the DNPR That May Be Used to Improve the Validity |
In the DFH, the PPV could be increased to 95.2% (95% CI: 90.6; 97.5) by restricting cases to individuals registered in the DFH with a pathogenic FH variant (158/166) (Table 3).
Evaluation of DLCN Parameters and Quality Indicators in the DFH
The validity of the individual items of the DLCN score registered in the DFH varied (Supplementary Table 3). Thus, PPVs were low for; first-degree relatives with tendon xanthoma and/or corneal arcus, or children < 18 years with LDL-C >95th percentile (8.3%) and for presence of premature peripheral/cerebral vascular disease (16.7%). The PPVs were moderate to high for; first degree relatives with premature coronary heart diseases or plasma LDL-C > 95% percentile (81.6%), presence of premature coronary heart disease (86.4%), corneal arcus < 45 years (66.7%), tendon xanthomas (77.8%), and highest measured plasma LDL-C (71.4–84.2%). The PPV was highest for the presence of a genetic FH variant (95.2%).
The completeness of the DLCN items varied between 10.0% for presence of premature history of peripheral and/or cerebral cardiovascular disease, to 85.0% for presence of premature coronary heart disease. Presence of genetic FH variants had a low to moderate completeness of 56.7%.
The DFH is used for nationwide quality assessment based on specified quality indicators.13,16 We calculated the proportion of individuals fulfilling quality indicators in patients registered in the DNPR (All: n = 800, verified n = 510) and the DFH (All FH cases: n = 383, verified FH cases: n = 318). The proportion of subjects that were genetically tested was higher for valid FH cases in the DNPR (95.3%) and DFH (98.1%) than for all FH cases in the DNPR (80%) or DFH (93.5%). More than 90% of patients had follow-up data available six months after they were registered with an FH diagnosis. However, only approximately 30% had received counselling by a clinical dietitian. The proportion of patients that reached their guideline recommended LDL-C target goal23 within six months after being registered with FH was 17.3% for all FH cases in the DNPR, 15.4% for all FH cases in the DFH, 14.2% for valid FH cases in the DNPR and 14.7% for valid FH cases in the DFH (Supplementary Table 4).
Discussion
Summary of Findings
The PPV of an FH diagnosis in the DNPR was 64% but restricting analysis to a primary diagnosis of FH and/or by restricting to diagnoses from departments of cardiology improved the validity to 69.4–71.0%. The PPV of registered diagnoses of heterozygous FH in the DNPR was 88%, but the diagnostic code was underused in the DNPR, covering only 56% of all likely pathogenic or pathogenic genetic FH variants identified. We found that the PPV of FH cases registered with a DLCN score ≥ 6 in the DFH was high (83%), but only 62% of valid FH cases from the DNPR were registered in the DFH. Furthermore, we validated the individual components of the DLCN scores registered in the DFH. The PPVs were high for presence of a likely pathogenic or pathogenic genetic FH variant and premature coronary heart disease. The PPVs were low for presence of premature peripheral arterial disease and first-degree relatives with FH stigmata or children with LDL-C above the 95th percentile for age and sex.
Explanations, Applicability and Perspectives
To our knowledge, this is the first validation study of registered FH diagnoses in the DNPR and the DFH. For comparison, other cardiac or vascular diagnoses in the DNPR have been validated with PPVs ranging between 45.9% (angina pectoris), 69.3% (stroke), 69.4% (peripheral arterial disease), 83.6% (heart failure) and 90.3% (acute myocardial infarction).24–27 Very limited data exist on the validity of FH diagnoses in registries in other countries. However, a study from the United States evaluated the concordance of Systematic Nomenclature of Medicine (SNOMED) and ICD-10 codes vs DLCN scores in the practices fusion electronically health records (EHR) database.28 The PPV of FH SNOMED codes in the EHR database was 18.7% for predicting a DLCN ≥ 6 in the EHR database.28 Several registries have been established for patients with FH, including the international Familial Hypercholesterolemia Study Collaboration registry.29,30 However, the vast majority of FH cases in this registry have not been validated, and importantly, a low validity of registered FH cases may dilute associations of interest in epidemiological studies and overestimate detection rates. The variation in validity between the different Danish regions might be due to regional variations in diagnostic practice and registrations, emphasizing the importance of a national harmonization.
The low validity for an FH diagnosis in our study may result in overestimation of the number of identified FH patients, and underestimation of the quality indicators used to improve FH management, which are fundamental for prioritization and optimal allocation of resources and treatments. Our findings highlight the necessity to investigate the validity of FH diagnoses and FH cases included in registries for the use of such data.
In addition, we evaluated the individual components of the DLCN score and specified quality indicators in the DFH. Interestingly, we found a high PPV of 95% for registered pathogenic FH variants, but our findings showed that registrations only covered 57% of all likely pathogenic or definite pathogenic results illustrating a high degree of underreporting. Presence of premature cardiovascular disease had a high PPV of 86% and a high completeness of 85% for an FH diagnosis. On the contrary, first-degree relatives with FH stigmata, or children with LDL-C above the 95% percentile for age and sex, had the lowest validity with a PPV of 8% illustrating the difficulties in obtaining information regarding family history. When using the DLCN parameters in registry research the PPVs and coverage should be taking into account.
The proportion of FH cases registered in the DFH fulfilling the specified quality indicators was comparable to the proportion of valid FH cases in the DFH fulfilling the specified quality indicators. However, less than 15% of valid FH patients reached their LDL-C targets which was surprising and warrant further research. Plausible explanations for the low percentage of patients achieving their LDL-C targets may include time delays in implementation of new guidelines, compliance issues and statin intolerance. Furthermore, access to initiation of treatment with PCSK9-inhibitors in Denmark is regulated according to specific criteria and there is currently a significant gap between recommended LDL-C target goals and access to treatment with PCSK9-inhibitors.
We developed algorithms to improve the validity of registered FH cases in the DNPR such as restricting any FH diagnosis to a primary diagnosis from a department of cardiology which improved the PPV, but only to 71%. Algorithms with restrictive case definitions could improve the validity with the trade-off being a substantial reduction in the number of cases available for analysis. The optimal FH case definition must have a high validity without a substantial reduction of sample size. The PPV of a diagnosis of heterozygous FH was 88%, but the diagnosis code was under-registered and covered only 56% of the genetic FH variants identified. In the DFH, restricting to FH cases registered with genetic FH, increased the PPV from 83% to 95%, but the case population was reduced from 383 to 166 FH cases. Thus, our findings emphasize the need for more focus on improvement of diagnostic coding of patients with FH. Some patients were registered with a heterozygous diagnosis code in the DNPR or with genetic FH in the DFH with a pathogenic variant in the ABCG5/ABCG8 genes (n = 6). These variants were not considered as valid genetic FH cases in this study.31 Genetic variants mimicking FH (n = 8) including genetic variants in the ApoE, ApoA5, LIPA, LPA gene variants and D362A variants were also not considered valid genetic FH cases.32–36
Strengths and Limitations
This study had strengths and limitations that warrant consideration. We retrieved a large nationwide random sample of registered FH diagnoses in the DNPR and subsequently validated registered FH cases in the DFH. The random sample from the DNPR corresponded to approximately 8% of all patients with an FH diagnosis in the DNPR as per 1st of July 2024.13 This approach allowed for detailed stratification analyses, which we used to develop algorithms that may be used to improve the validity of case definitions of FH for future quality assessment and research. We collected clinical data from medical records with data retrieved by lipid specialists using pre-specified validation sheets, which was used as the golden standard in our validation. Inadequate or missing information in the medical records may have resulted in misclassification of true FH cases thus underestimating the PPVs, however, we used the best available validation standard employed in validation studies.11,37 The use of genetic testing for FH in the Danish lipid clinics has increased over the recent years.38 Nearly 60% of patients referred to Danish lipid clinics on suspicion of FH are genetically tested.38 A study showed that genetic testing increased the proportion of patients diagnosed with FH from 22% to 37% compared to diagnostics based on clinical criteria alone.38 However, it should be emphasized that a negative genetic test does not rule out FH, and that the quality of genetic test arrays varies. Furthermore, we acknowledge that the approach for genetic testing used in Denmark may not be feasible in many countries worldwide.
We retrieved information on FH diagnoses after the DFH was established in 2020 and were therefore not able to assess temporal trends in validity over time and we did not perform an internal cross validation. Also, our sampling strategy did not allow for calculation of sensitivity, specificity, or negative predictive values as all individuals had been registered with an FH diagnosis.
Conclusions
The positive predictive value of an FH diagnosis in the DNPR was low (64%), but algorithms restricting analysis to a primary diagnosis of FH from a department of cardiology improved the validity (71%). The PPV of registered diagnoses of heterozygous FH in the DNPR was high (88%), but the diagnostic code was underreported (56%). The PPV of FH cases registered with a DLCN score ≥ 6 in the DFH was high (83%), but only 62% of valid FH cases from the DNPR were registered in the DFH. Our findings support the importance of validation and harmonization of correct diagnostic coding of patients with FH. Finally, less than 15% of validated cases reached their guideline-recommended LDL-C target, underscoring the need to explore potential barriers to effective goal attainment, reducing the future burden of premature cardiovascular disease associated with FH.
Abbreviations
ABCG5, ATP Binding Cassette Subfamily G Member 5; ABCG8, ATP Binding Cassette Subfamily G Member 8; ApoA5, Apolipoprotein A5; ApoB, Apolipoprotein B; ApoE, Apolipoprotein E; ASCVD, Atherosclerotic Cardiovascular Disease; CAD, Coronary Artery Disease; CI, Confidence Interval; CPR, Central Person Registry; DE780B, ICD-10 Familial Hypercholesterolemia diagnostic code; DE780B1, ICD-10 Heterozygous Familial Hypercholesterolemia diagnostic code; DE780B2 ICD-10 Homozygous Familial Hypercholesterolemia diagnostic code; DFH, Danish Familial Hypercholesterolemia Registry; DHQI, Danish Healthcare Quality Institute; DLCN, Dutch Lipid Clinical Network; DNPR, Danish National Patients Registry; EHR, Electronically Health Record; FH, Familial hypercholesterolemia; ICD-8, International Statistical Classification of Diseases 8th Revision; ICD-10, International Statistical Classification of Diseases 10th Revision; IQR, Inter Quartile Range; LDL-C, Low-density lipoprotein cholesterol; LDLR, Low density lipoprotein receptor; LIPA, Lysosomal acid lipase; Lp(a), Lipoprotein a; N, Number; OPEN, Open Patient Explorative Network; PCSK9, Proprotein-convertase-subtilisin/kexin-type 9; PPV, Positive Predicitive Value; REDcapTM, Research Electronic Data CaptureTM; SNOMED, Systematic Nomenclature of Medicine.
Reporting, Data Protection Statement and Data Availability
This study was reported according to a Modified STARD guideline for validation studies.22 The approval by the Regional Council in the Region of Southern Denmark (23/19548) covers access to medical records. All data complied with general data protection regulations and privacy regulations according to Danish law. According to Danish law, our approval does not cover sharing of data from the medical record. Data from the registries can be requested at https://forskningsadgang.sundk.dk/.
Acknowledgments
We thank lipid clinic staff and the Danish FH Study Group for the valuable contribution, the Danish Familial Hypercholesterolemia Registry and the DHQI for access to data and Open Patient Data Explorative Network (OPEN) for use of data infrastructure. The abstract of this paper as well as data regarding treatment quality of FH patients were presented at the European Society of Cardiology Conference 2025 as two poster presentations based on interim findings. The poster’s abstracts (Validation) and Treatment quality were published as a supplement online in European Heart Journal (Volume 46 Issue Supplemental 1).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
A Healthier Southern Denmark Competition - Odense University Hospital and the Region of Southern Denmark (23/49277), Region of Southern Denmark PhD grant (2023-0008). The funding did not influence completion of this study.
Disclosure
Dr Jakob Knold reports personal fees or grants from Amgen, Novartis, Novo Nordisk, outside the submitted work. Dr Christian Bork reports grants from The Karen Elise Jensens Foundation, during the conduct of the study. Dr Mette Bertelsen reports personal fees from Norvartis, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Schmidt EB, Hedegaard BS, Retterstol K. Familial hypercholesterolaemia: history, diagnosis, screening, management and challenges. Heart. 2020;106(24):1940–13. doi:10.1136/heartjnl-2019-316276
2. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188. doi:10.1093/eurheartj/ehz455
3. Collaboration EASFHS. Global perspective of familial hypercholesterolaemia: a cross-sectional study from the EAS familial hypercholesterolaemia studies collaboration (FHSC). Lancet. 2021;398(10312):1713–1725. doi:10.1016/S0140-6736(21)01122-3
4. Mulverstedt S, Hildebrandt PR, Prescott E, Heitmann M. Screening for potential familial hypercholesterolaemia in general practice: an observational study on prevalence and management. BJGP Open. 2021;5(2). doi:10.3399/bjgpopen20X101142
5. Rerup SA, Rorth R, Bang LE, et al. Room for improvement: initiation of lipid-lowering treatment and achievement of lipid target levels-a Danish registry-based study. Eur Heart J Qual Care Clin Outcomes. 2021;7(2):181–188. doi:10.1093/ehjqcco/qcaa004
6. Beheshti SO, Madsen CM, Varbo A, Nordestgaard BG. Worldwide prevalence of familial hypercholesterolemia: meta-analyses of 11 million subjects. J Am Coll Cardiol. 2020;75(20):2553–2566. doi:10.1016/j.jacc.2020.03.057
7. Slack J. Risks of ischaemic heart-disease in familial hyperlipoproteinaemic states. Lancet. 1969;2(7635):1380–1382. doi:10.1016/s0140-6736(69)90930-1
8. Luirink IK, Wiegman A, Kusters DM, et al. 20-Year follow-up of statins in children with familial hypercholesterolemia. N Engl J Med. 2019;381(16):1547–1556. doi:10.1056/NEJMoa1816454
9. Cuchel M, Raal FJ, Hegele RA, et al. 2023 update on european atherosclerosis society consensus statement on homozygous familial hypercholesterolaemia: new treatments and clinical guidance. Eur Heart J. 2023;44(25):2277–2291. doi:10.1093/eurheartj/ehad197
10. Tromp TR, Hartgers ML, Hovingh GK, et al. Worldwide experience of homozygous familial hypercholesterolaemia: retrospective cohort study. Lancet. 2022;399(10326):719–728. doi:10.1016/S0140-6736(21)02001-8
11. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish national patient registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
12. Bundgaard H. Databasen for familiær hyperkolesterolæmi årsrapport 2023. [The Danish familial hypercholesterolemia registry yearly report 2023] Aarhus: regionernes Kliniske Kvalitetsudviklingsprogram (RKKP);2023. Available from: https://www.sundhed.dk/content/cms/33/123533_dfh_aarsrapport-2022_230309_offentliggjort-version.pdf.
13. Bork C, Bundgaard H, Snoer M, et al. The Danish familial hypercholesterolemia registry: monitoring of diagnostics, detection, and treatment quality in denmark. Atherosclerosis. 2024;395.
14. Benn M, Watts GF, Tybjaerg-Hansen A, Nordestgaard BG. Mutations causative of familial hypercholesterolaemia: screening of 98 098 individuals from the copenhagen general population study estimated a prevalence of 1 in 217. Eur Heart J. 2016;37(17):1384–1394. doi:10.1093/eurheartj/ehw028
15. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
16. Bundgaard H. Databasen for familiær hyperkolesterolæmi årsrapport 2024 [The Danish familial hypercholesterolemia registry yearly report 2024] aarhus: Regionernes Kliniske Kvalitetsudviklingsprogram (RKKP);2024. Available from: https://www.sundk.dk/media/4droxpqw/dfh-aarsrapport-2024.pdf.
17. Andersen TF, Madsen M, Jorgensen J, Mellemkjoer L, Olsen JH. The Danish national hospital register. A valuable source of data for modern health sciences. Dan Med Bull. 1999;46(3):263–268.
18. Uggerby C, Kristensen S, Mackenhauer J, et al. From accreditation to quality improvement-the Danish national quality programme. Int J Qual Health Care. 2021;33(2). doi:10.1093/intqhc/mzab071
19. Leigh S, Futema M, Whittall R, et al. The UCL low-density lipoprotein receptor gene variant database: pathogenicity update. J Med Genet. 2017;54(4):217–223. doi:10.1136/jmedgenet-2016-104054
20. Schmidt EBHF, Kanstrup HL. Familiær hyperkolesterolæmi - holdningspapir. Danish society of cardiology. [Familial Hypcercholesterolemia holdningspapir - Position Paper]. Copenhagen: Danish Society of Cardiology; 2024. Available from: https://www.cardio.dk/media/com_reditem/files/customfield/item/8155/75510f748b88359bab6b9d7193dea19421cc0df8.pdf.
21. Validation of the National familial hypercholesterolemia database [homepage on the internet]. Odense: Odense University Hospital, Open Patient data Explorative Network; 2023. Available from: https://open.rsyd.dk/OpenProjects/openProject.jsp?openNo=1927&lang=en.
22. Benchimol EI, Manuel DG, To T, Griffiths AM, Rabeneck L, Guttmann A. Development and use of reporting guidelines for assessing the quality of validation studies of health administrative data. J Clin Epidemiol. 2011;64(8):821–829. doi:10.1016/j.jclinepi.2010.10.006
23. Bork C, Henriksen FLKH, Bang LE, Mortensen MB, Heitmann M, Mouridsen MR. Dyslipidæmi - national behandlingsvejledning [dyslipidemia - national guideline]. Danish society of cardiology. Available from: https://nbv.cardio.dk/dyslipidaemi.
24. Bork CS, Al-Zuhairi KS, Hansen SM, Delekta J, Joensen AM. Accuracy of angina pectoris and acute coronary syndrome in the Danish national patient register. Dan Med J. 2017;64(5).
25. Luhdorf P, Overvad K, Schmidt EB, Johnsen SP, Bach FW. Predictive value of stroke discharge diagnoses in the Danish national patient register. Scand J Public Health. 2017;45(6):630–636. doi:10.1177/1403494817716582
26. Lasota AN, Overvad K, Eriksen HH, Tjonneland A, Schmidt EB, Gronholdt MM. Validity of peripheral arterial disease diagnoses in the Danish national patient registry. Eur J Vasc Endovasc Surg. 2017;53(5):679–685. doi:10.1016/j.ejvs.2016.12.031
27. Delekta J, Hansen SM, AlZuhairi KS, Bork CS, Joensen AM. The validity of the diagnosis of heart failure (I50.0-I50.9) in the Danish national patient register. Dan Med J. 2018;65(4).
28. Mues KE, Bogdanov AN, Monda KL, Yedigarova L, Liede A, Kallenbach L. How well can familial hypercholesterolemia be identified in an electronic health record database? Clin Epidemiol. 2018;10:1667–1677. doi:10.2147/CLEP.S176853
29. Amerizadeh A, Javanmard SH, Sarrafzadegan N, Vaseghi G. Familial Hypercholesterolemia (FH) registry worldwide: a systematic review. Curr Probl Cardiol. 2022;47(10):100999. doi:10.1016/j.cpcardiol.2021.100999
30. EEAS FH Collaboration, Vallejo-Vaz AJ, Akram A, et al. Pooling and expanding registries of familial hypercholesterolaemia to assess gaps in care and improve disease management and outcomes: rationale and design of the global EAS familial hypercholesterolaemia studies collaboration. Atheroscler Suppl. 2016;22:1–32. doi:10.1016/j.atherosclerosissup.2016.10.001
31. Reeskamp LF, Volta A, Zuurbier L, Defesche JC, Hovingh GK, Grefhorst A. ABCG5 and ABCG8 genetic variants in familial hypercholesterolemia. J Clin Lipidol. 2020;14(2):207–217e7. doi:10.1016/j.jacl.2020.01.007
32. Abifadel M, Boileau C. Genetic and molecular architecture of familial hypercholesterolemia. J Intern Med. 2023;293(2):144–165. doi:10.1111/joim.13577
33. De Castro-Oros I, Cenarro A, Tejedor MT, et al. Common genetic variants contribute to primary hypertriglyceridemia without differences between familial combined hyperlipidemia and isolated hypertriglyceridemia. Circ Cardiovasc Genet. 2014;7(6):814–821. doi:10.1161/CIRCGENETICS.114.000522
34. Medeiros AM, Alves AC, Miranda B, Chora JR, Bourbon M. investigators of the Portuguese FHS. Unraveling the genetic background of individuals with a clinical familial hypercholesterolemia phenotype. J Lipid Res. 2024;65(2):100490. doi:10.1016/j.jlr.2023.100490
35. Clarke R, Peden JF, Hopewell JC, et al. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med. 2009;361(26):2518–2528. doi:10.1056/NEJMoa0902604
36. Zeng XH, Xia XM, Lingle CJ. Divalent cation sensitivity of BK channel activation supports the existence of three distinct binding sites. J Gen Physiol. 2005;125(3):273–286. doi:10.1085/jgp.200409239
37. Pedersen AB, Johnsen SP. Vejledning for validering af data fra kliniske kvalitetsdatabaser regionernes kliniske kvalitetsudviklings program [Guideline for validation of data from clinical quality databases]. aarhus: Regionernes Kliniske Kvalitetsudviklingsprogram (RKKP);2017. Available from: https://www.rkkp.dk/siteassets/de-kliniske-kvalitetsdatabaser/projekter/valideringmanuel_rkkp_-final_06062017.pdf.
38. Hedegaard BS, Bork CS, Kanstrup HL, et al. Genetic testing increases the likelihood of a diagnosis of familial hypercholesterolaemia among people referred to lipid clinics: Danish national study. Atherosclerosis. 2023;373:10–16. doi:10.1016/j.atherosclerosis.2023.04.003
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Danish Heart Failure Registry: A Validation Study of Content
Andersen C, Schjødt I, Nakano A, Johnsen SP, Egstrup K, Løgstrup BB
Clinical Epidemiology 2022, 14:1585-1594
Published Date: 28 December 2022
Positive Predictive Value of Non-Traumatic Bleeding Diagnoses in the Danish National Patient Register
Thaarup M, Nielsen PB, Olesen AE, Bitsch Poulsen M, Larsen TB, Wittström F, Overvad TF
Clinical Epidemiology 2023, 15:493-502
Published Date: 28 April 2023
High Validity and Completeness of the Septoplasty Surgical Procedure Code in the Danish National Patient Registry
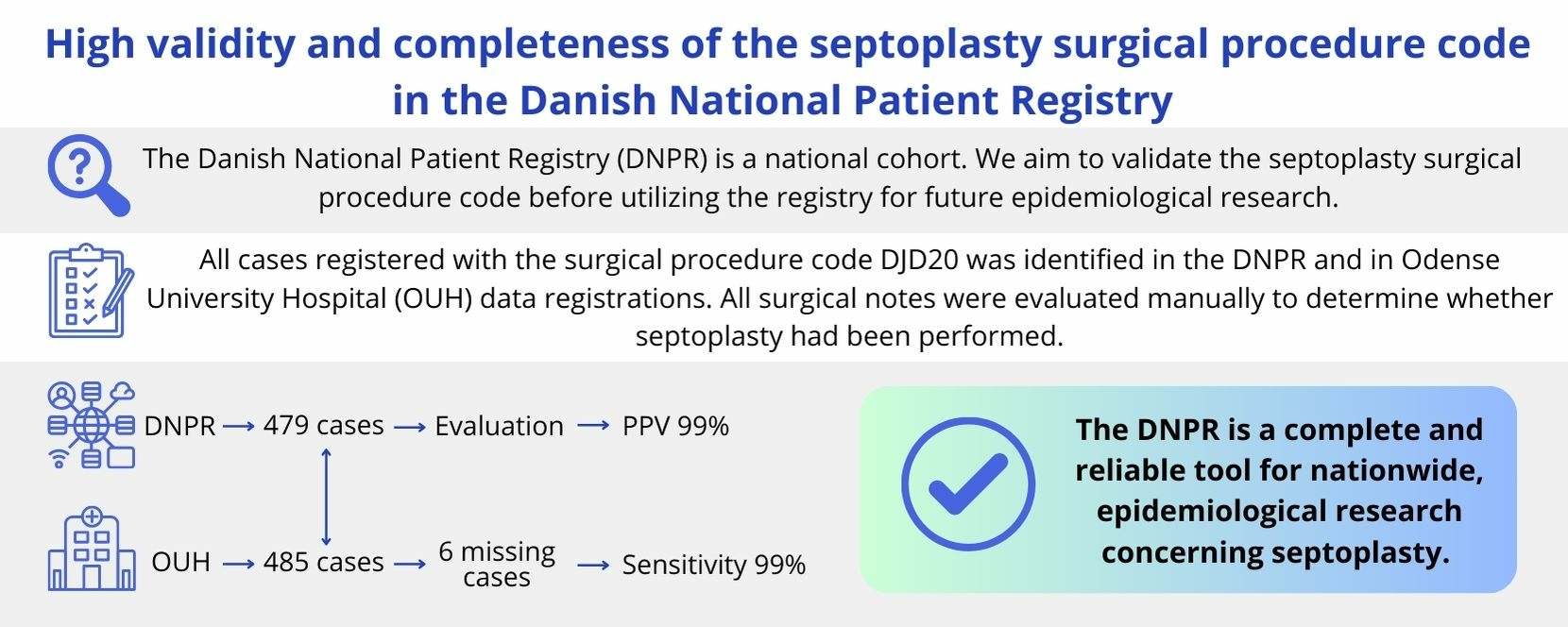
Bredahl JØ, Rønnegaard AB, Larsen KS, Kjeldsen AD
Clinical Epidemiology 2025, 17:435-440
Published Date: 28 April 2025