Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Predictive Value of Age-Adjusted Charlson Comorbidity Index on Survival Outcomes of Hepatocellular Carcinoma Patients with Comorbidities Undergoing Radiofrequency Ablation
Authors Yan Y ![]() , Xiao S
, Xiao S ![]() , Xia F, Bi H, Tang C, Feng K, Ma K, Wang Q
, Xia F, Bi H, Tang C, Feng K, Ma K, Wang Q ![]()
Received 30 January 2026
Accepted for publication 8 April 2026
Published 16 April 2026 Volume 2026:13 599999
DOI https://doi.org/10.2147/JHC.S599999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ahmed Kaseb
Yuzheng Yan,1,* Sijie Xiao,1,* Feng Xia,1 Huaqiang Bi,1 Chunlin Tang,2 Kai Feng,1 Kuansheng Ma,1 Qiang Wang3
1Department of Hepatobiliary Surgery, The First Affiliated Hospital (Southwest Hospital) of Army Medical University, Chongqing, People’s Republic of China; 2Department of Ultrasound, The First Affiliated Hospital (Southwest Hospital) of Army Medical University, Chongqing, People’s Republic of China; 3Department of Clinical Science, Intervention and Technology (CLINTEC), Karolinska Institutet, Stockholm, Sweden
*These authors contributed equally to this work
Correspondence: Kuansheng Ma, Department of Hepatobiliary Surgery, The First Affiliated Hospital (Southwest Hospital) of Army Medical University, Chongqing, People’s Republic of China, Email [email protected] Kai Feng, Department of Hepatobiliary Surgery, The First Affiliated Hospital (Southwest Hospital) of Army Medical University, Chongqing, People’s Republic of China, Email [email protected]
Purpose: This study aimed to explore the predictive value of Age-Adjusted Charlson Comorbidity Index (ACCI) on survival outcomes in patients with hepatocellular carcinoma (HCC) and comorbidities undergoing radiofrequency ablation (RFA).
Materials and Methods: This study is a retrospective, single-center study which included 158 patients with HCC newly diagnosed at our center from January 2015 to December 2021 who had comorbidities prior to RFA treatment. Patients were divided into two groups (≤ 4 and > 4) according to the optimal cutoff value of ACCI determined by X-tile analysis based on overall survival (OS), and comprehensive clinical, laboratory, and tumor characteristic data were collected. The primary endpoints were OS and recurrence-free survival (RFS), analyzed using the Kaplan-Meier method and Cox proportional hazards model.
Results: Patients in the high ACCI group (> 4) were independently associated with worse OS and RFS compared to those in the low ACCI group (≤ 4). Multivariate Cox analysis confirmed that ACCI > 4 was an independent risk factor for both OS and RFS, with hazard ratios (HR) of 2.07 and 2.05, respectively. In addition to ACCI, other independent predictors for worse OS included tumor max-diameter (HR: 1.69, P < 0.001) and elevated level of preoperative α-fetoprotein (HR: 1.91, P = 0.007), while preoperative albumin (HR: 0.93, P=0.001) was a significant protective factor for OS. For RFS, significant risk factors included tumor max-diameter (HR: 1.79, P < 0.001) and prothrombin time ≥ 13 seconds (HR: 2.38, P = 0.001).
Conclusion: ACCI may serve as a useful prognostic predictor for survival outcomes in HCC patients with comorbidities undergoing RFA.
Keywords: hepatocellular carcinoma, radiofrequency ablation, comorbidities, Age-Adjusted Charlson Comorbidity Index, survival
Introduction
According to GLOBOCAN 2022 data, primary liver cancer ranks as the sixth most common malignant tumor globally, with approximately 865,000 new cases annually, accounting for 4.3% of all new cancer cases worldwide. Simultaneously, it ranks as the third leading cause of cancer-related deaths worldwide, with approximately 758,000 fatalities annually, accounting for 7.8% of all cancer deaths. This indicates a high mortality-to-incidence ratio for liver cancer, reflecting its relatively poor prognosis. Hepatocellular carcinoma (HCC) is the most common type of liver cancer.1
The latest international guidelines for HCC treatment list ablation therapy alongside liver resection and liver transplantation as curative treatment options. Among ablation therapies, radiofrequency ablation (RFA) is widely used. Compared to surgical resection, RFA presents distinct advantages for HCC patients with poor physical condition or comorbidities unsuitable for resection. It delivers reliable efficacy, is minimally invasive and cost-effective, has minimal impact on liver function, and carries fewer complications. For patients with early-stage HCC, RFA can achieve similar efficacy to surgical resection.2–4
In fact, the burden of preoperative comorbidities has been widely recognized as a prognostic factor affecting postoperative survival rates for various solid tumors.5–13 For HCC patients who opt for RFA due to chronic comorbidities rendering them unsuitable for surgical resection, stratifying the risk of comorbidities prior to treatment is critically important.
As a commonly used clinical indicator for stratifying the risk of comorbidities, Charlson Comorbidity Index (CCI) was developed by Charlson et al based on research into past medical records.14 Subsequently, age was incorporated as an adjusted factor, with one point added for every decade above 40 years old, thereby forming the Age-Adjusted Charlson Comorbidity Index (ACCI).15 Currently, ACCI has demonstrated predictive value in the prognosis of various cancer treatment.6–13
However, although ACCI has been validated in HCC resection, RFA for other malignancies, and various oncologic settings, its prognostic value specifically in HCC patients undergoing RFA remains less extensively studied. Understanding the relationship between comorbidity burden and postoperative outcomes in this specific population is important for guiding risk stratification and individualized management. Therefore, this study aims to provide incremental evidence for the predictive value of ACCI in HCC patients with comorbidities treated with RFA.
Materials and Methods
Patients
This is a retrospective single center study. Clinical information of HCC patients who underwent RFA treatment between January 2015 and December 2021 in the Department of Hepatobiliary Surgery at the First Affiliated Hospital of Army Medical University was collected from the hospital’s electronic medical record system. Inclusion criteria are: 1) age ≥18 years; 2) newly diagnosed with primary HCC according to AASLD guidelines; 3) solitary tumor diameter ≤5 cm or 2–3 tumors with the largest ≤3 cm; 4) preoperative diagnosis of extrahepatic comorbidities (disease categories referenced in ACCI).15 Exclusion criteria are: 1) RFA combined with other treatments; 2) Palliative RFA therapy; 3) Insufficient follow-up information; 4) Incomplete RFA treatment records; 5) Receiving liver transplantation after RFA (Figure 1).
 |
Figure 1 Flowchart of patient selection. |
This retrospective, single-center study has been approved by the Ethics Committee of the First Affiliated Hospital (Southwest Hospital) of Army Medical University, Chongqing, China (No. (B)KY2025048), and complies with the standards of the Declaration of Helsinki and local ethical guidelines. All personal identifying information was anonymized before analysis to protect patient privacy. Informed consent was waived by the Ethics Committee of the First Affiliated Hospital of Army Medical University due to the retrospective nature of the study and anonymized data.
Clinical Data
Demographic characteristics included sex, age and body mass index (BMI). Imaging findings included number of tumors and tumor maximum diameter. Laboratory test results encompassed total bilirubin (TB), serum albumin (ALB), aspartate transaminase (AST), alanine aminotransferase (ALT), prothrombin time (PT), platelet (PLT), alkaline phosphatase (ALP), α-fetoprotein (AFP), hepatitis B surface antigen (HBsAg), anti-hepatitis C virus (Anti-HCV). Additionally, tumor staging conducted in accordance with the China Liver Cancer Staging System (CNLC) criteria, and Child-Pugh scores reflecting liver function were also documented.
Patient Comorbidities
The Age-adjusted Charlson Comorbidity Index extends the original Charlson Comorbidity Index by incorporating age as an additional prognostic factor.15 In specific, 1 point is assigned for comorbidities of myocardial infarction, congestive heart failure, peripheral vascular disease, cerebral vascular disease, dementia, chronic pulmonary disease, connective tissue disease, ulcer disease, mild liver disease and diabetes without end organ damage, 2 points for hemiplegia, moderate/severe renal disease, diabetes with end-organ disease, solid tumor, leukemia and lymphoma, 3 points for moderate/severe liver disease, and 6 points for metastatic solid tumor and acquired immunodeficiency syndrome. One point is added for every decade above 40 years, allowing the score to better estimate long-term mortality risk of the patients (Supplementary Table S1). ACCI is widely used to quantify comorbidity burden in clinical research and outcome prediction.6–13 This study adopted ACCI for quantifying patient comorbidities. Each patient was assigned an ACCI score based on their preoperative diagnosis.
Treatment Procedures
All radiofrequency ablation procedures were performed percutaneously under real-time contrast-enhanced ultrasound (CEUS) guidance by three experienced hepatobiliary surgeons, with all cases undergoing monitored anesthesia. Under ultrasound guidance, the largest section of the tumor was selected and one or two electrode needles were punctured directly into the lesion. The ablation power was set at 120 watts and the working time was 3min. When the tumor was larger than 3cm and smaller than 5cm, two ablation needles were used for puncture and ablation. The ablation power was 180 watts and the working time was 5min. Needle-track ablation was performed when the electrode was withdrawn. Each ablation targeted a safety margin of at least 0.5 cm beyond the tumor boundary. Postoperative CEUS was repeated within 20 minutes to assess ablation extent; residual tumor was immediately re-ablated to achieve complete tumor destruction. On the second postoperative day, a repeat CEUS or contrast-enhanced upper abdominal computed tomography (CT) scan was performed to further confirm the absence of residual lesions and measure the size of the destroyed area (using the maximum cross-sectional diameter). If residual lesions were detected, additional ablation was performed as soon as possible based on the patient’s overall condition. All procedures were performed following a standardized RFA protocol, with each surgeon adhering to consistent electrode placement, ablation power and duration, target safety margin, and postoperative imaging assessment, ensuring reproducibility across operators. If no residual lesions were identified on postoperative imaging, the ablation was considered complete.
Patient Follow-Up
Ablation efficacy was evaluated via Gd-EOB-DTPA-enhanced magnetic resonance imaging (EOB-MRI) or contrast-enhanced upper abdominal CT one month after ablation. Subsequently, rechecked relevant laboratory indicators and imaging examinations every 3 months to assess treatment outcomes. Statistics included overall survival (OS, defined as the time from the end of treatment until death or the date of the last follow-up) and recurrence-free survival (RFS, defined as the time from the end of treatment until tumor recurrence or metastasis; patients who died without documented recurrence were censored at the time of death). The follow-up cutoff date was December 31, 2023.
Statistical Methods
Baseline characteristics were summarized using descriptive statistics. Categorical variables were expressed as counts and percentages, while continuous variables were expressed as medians with interquartile ranges (IQR). Group comparisons were performed using Pearson’s chi-squared test or Fisher’s exact test for categorical variables and the Mann–Whitney U-test for continuous variables. Survival outcomes, including OS and RFS, were estimated using the Kaplan–Meier method and compared using the Log rank test. Univariate and multivariable Cox proportional hazards models were used to identify prognostic factors. Candidate variables were selected based on both statistical significance in univariate analysis (P < 0.05) and clinical relevance. Age was excluded from the multivariable model because it is a component of ACCI. Child-Pugh classification was excluded to avoid redundancy with ACCI liver disease scoring, while laboratory indicators of liver function (ALB, PT, AST, ALT) were retained. Stepwise Cox regression based on the Akaike Information Criterion (AIC) was applied to select the final model. Variance inflation factors (VIFs) were calculated to assess multicollinearity, and all variables showed low collinearity (all VIF < 5). Proportional hazards assumptions were evaluated using Schoenfeld residuals, with no evidence of significant violation. Model performance was assessed using Harrell’s concordance index (C-index), and internal validation was performed using bootstrap resampling with 1,000 iterations. Continuous variables were dichotomized according to clinically established reference thresholds commonly used in clinical practice.16 The optimal cutoff value of ACCI was determined using X-tile software based on OS and was subsequently applied to RFS analysis. All statistical analyses were performed using R (version 4.3.1), and a two-sided P value < 0.05 was considered statistically significant. No significant missing data were observed; therefore, complete-case analysis was performed.
Results
Baseline Data of Patients
This study included 158 patients and the patients’ baseline characteristics were recorded in Table 1. There were 124 males (78.5%) and 34 females (21.5%), with a median age of 60.5 (IQR: 53.0–68.0) years. Among the 158 patients, 122 (77.2%) were HBsAg-positive. Two patients had hepatitis C, and 15 had alcoholic liver disease. Thirteen patients had total bilirubin ≥34 μmol/L, 43 had AST ≥42 U/L, 40 had ALT ≥42 U/L, 35 had PT ≥13 seconds, and 58 had AFP ≥20 ng/mL. The median tumor maximum diameter was 2.4 cm (IQR: 1.8–3.1). The median tumor number was 1. The median ACCI score was 4. X-tile analysis also identified 4 as the optimal cutoff value for ACCI based on OS. The median follow-up time for the cohort was 63 months using the reverse Kaplan–Meier method (IQR, 47.0–88.0 months). Baseline characteristics stratified by ACCI group are presented in Table 2, patients with higher ACCI scores were older and had poorer liver function, as reflected by lower albumin levels and platelet counts. In contrast, tumor-related characteristics, including tumor size and number, were comparable between the two groups.
 |
Table 1 Demographic and Clinical Characteristics of Patients |
 |
Table 2 Baseline Characteristics Stratified by ACCI Group |
Comorbidities Distribution Among Patients
The comorbidities distribution of all included patients is summarized in Table 3. In the 1 score group cohort, diabetes without end-organ damage was the most common comorbidity, affecting 103 patients (65.2%). Mild liver disease, chronic lung disease, and peptic ulcer disease followed, with 82 cases (51.9%), 29 cases (18.4%), and 18 cases (11.4%), respectively. In the 2 scores group, 13 patients (8.2%) had moderate-to-severe renal disease, 4 patients (2.5%) had diabetes with organ damage, and 1 patient each (0.6%) had other solid tumor and leukemia. In the 3 scores group, 38 patients (24.1%) had moderate-to-severe liver disease. No patients were assigned a 6-point.
 |
Table 3 Weighted Index of Comorbidities in the Age-Adjusted Charlson Comorbidity Index and Distribution of Patients’ Comorbidities |
ACCI and OS
To evaluate the prognostic predictive capacity of ACCI, this study grouped patients according to the optimal cutoff value of ACCI determined by X-tile analysis and employed Kaplan-Meier curves to illustrate postoperative OS and RFS. During follow-up, 47.5% (75/158) of the entire cohort died. The 1-, 3-, and 5-year OS rates following RFA were 91.8%, 71.1%, and 56.4%, respectively. The median OS was 69 months (95% CI:54–91) (Figure 2A).
 |
Figure 2 Kaplan-Meier curve of overall survival for all included patients (A) and different ACCI groups (B), ACCI ≤4 vs. ACCI >4). Abbreviations: ACCI, Age-adjusted Charlson Comorbidity Index; OS, overall survival. |
Patients were categorized into low ACCI (≤4) and high (>4) ACCI groups. The 1-year OS rates for these two groups were 96.0% and 84.7%, respectively; 3-year OS rates were 78.9% and 58.1%; and 5-year OS rates were 65.5% and 40.4%, a significant difference was observed between the two groups (P=0.00054, Figure 2B).
ACCI and RFS
We evaluated the RFS for the entire cohort and found that 71.5% (113/158) of patients experienced recurrence or metastasis during postoperative follow-up. The 1-, 3-, and 5-year RFS rates for the entire group were 57.0%, 36.0%, and 30.7%, respectively, with a median RFS of 20 months (95% CI:12–28) (Figure 3A). The 1-year RFS rates for the low and high ACCI groups were 64.6% and 44.1%, respectively. The 3-year RFS rates were 43.9% and 22.6%, and the 5-year RFS rates were 36.2% and 22.6%. A significant difference existed between the two groups (ACCI ≤4 vs. ACCI >4), with a P value of 0.006 (Figure 3B).
 |
Figure 3 Kaplan-Meier curve of recurrence-free survival for all included patients (A) and different ACCI groups (B), ACCI ≤4 vs. ACCI >4). Abbreviations: ACCI, Age-adjusted Charlson Comorbidity Index; RFS, recurrence-free survival. |
Predictive Factors of OS and RFS
Utilizing the Cox proportional hazards model, we conducted univariate and multivariate analyses for postoperative overall survival and recurrence-free survival to define predictive factors. For OS, multivariate analysis indicated that tumor max-diameter (HR: 1.69, 95% CI: 1.35–2.11, P < 0.001) and AFP (HR: 1.91, 95% CI: 1.19–3.07, P = 0.007) were risk factors for OS following RFA. ACCI > 4 (HR: 2.07, 95% CI: 1.29–3.33, P=0.003) was independently associated with worse OS. Preoperative albumin (HR: 0.93, 95% CI: 0.89–0.97, P=0.001) was an independent protective factor (Table 4). Age, significant in univariate analysis, was excluded due to collinearity with ACCI. The model showed good discrimination with a Harrell’s C-index of 0.713 and internal validation by bootstrap (1,000 iterations) yielded a mean C-index of 0.720, 95% CI: 0.650–0.785.
 |
Table 4 Univariate and Multivariate Cox Analysis for Overall Survival |
For RFS, multivariate analysis indicated that tumor maximum diameter (HR: 1.79, 95% CI: 1.45–2.22, P < 0.001), PT ≥ 13 seconds (HR: 2.38, 95% CI: 1.43–3.94, P = 0.001), and ACCI >4 (HR: 2.05, 95% CI: 1.28–3.28, P = 0.003) were independently associated with worse postoperative RFS (Table 5). The model demonstrated good discrimination with Harrell’s C-index of 0.728 (SE = 0.033). Internal validation using 1,000 bootstrap iterations yielded a mean C-index of 0.732 (95% CI 0.663–0.794).
 |
Table 5 Univariate and Multivariate Cox Analysis for Recurrence-Free Survival |
Discussion
In this study, we investigated the distribution of comorbidities among HCC patients undergoing RFA treatment and evaluated the prognostic performance of ACCI score. Cox analysis revealed that ACCI was independently associated with OS and RFS in patients with hepatocellular carcinoma undergoing radiofrequency ablation. The cutoff value of ACCI was determined using X-tile analysis, which has been widely applied to identify optimal prognostic thresholds in survival studies. Notably, patients with an ACCI >4 exhibited significantly higher risk of death and tumor recurrence compared to those with lower scores.
As shown in the baseline comparison (Table 2), patients with higher ACCI scores tended to be older and exhibited poorer liver function, which is consistent with the components incorporated in the ACCI. These differences reflect the underlying clinical characteristics captured by the index rather than representing unexpected imbalance. Importantly, multivariable Cox regression analysis was performed to adjust for potential confounders, and ACCI remained independently associated with survival outcomes, supporting its prognostic value beyond individual clinical factors. Therefore, the effect of ACCI should be interpreted as a composite measure reflecting both age and comorbidity burden, rather than an independent comorbidity-only effect.
As shown in Table 3, diabetes emerged as the most prevalent comorbidity in the study cohort. Research has indicated that diabetes is a risk factor for HCC development,1 while liver diseases—represented by HCC—can also cause impaired glucose metabolism.17 Next in prevalence were varying degrees of liver disease. The definition of liver disease severity primarily depended on the presence of decompensated liver function manifestations such as portal hypertension, history of variceal bleeding, ascites, or hepatic encephalopathy.15 The pathophysiological changes associated with hepatocellular carcinoma can explain the high incidence of liver disease across different severity levels.18,19 Chronic pulmonary disease and peptic ulcer disease follow closely. Chronic pulmonary disease included COPD and bronchiectasis patients. The high incidence of peptic ulcer disease may be related to concomitant portal hypertension and coagulation abnormalities in HCC patients.20,21
As shown in Table 4, multivariate Cox analysis of overall survival revealed that tumor max-diameter (HR = 1.69 CI: 1.35–2.11 P< 0.001) and higher AFP level (HR = 1.91 CI: 1.19–3.07 P= 0.007) are risk factors for OS following RFA. Potential reasons for the association between larger tumor max-diameter and increased risk include: First, a larger tumor means a more abundant surrounding vascular bed, resulting in more heat dissipation through blood flow during RFA treatment (heat sink effect), which consequently impacts ablation temperature and efficacy.22 Second, tumor lesions exhibit irregular shapes, and since conventional RFA is typically guided by two-dimensional ultrasound and/or CT imaging, a larger tumor increase the risk of failing to precisely position the ablation electrode at the lesion’s three-dimensional center, leading to inadequate ablation in other planes.23 Third, a larger tumor may generate more water vapor during ablation, hindering real-time visualization of residual cancer tissue within the lesion.24 Higher AFP levels were associated with worse OS. This may be attributed to tumors with higher AFP level being more aggressive, more prone to micro-metastasis, and less responsive to treatment.25 Preoperative albumin (HR = 0.93 CI: 0.89–0.97 P= 0.001) served as a significant protective factor, highlighting the importance of the patient’s nutritional status for long-term prognosis.26
As shown in Table 5, multivariate Cox analysis of recurrence-free survival revealed that tumor max-diameter (HR = 1.79 CI: 1.45–2.22 P< 0.001) and PT (HR = 2.38 CI: 1.43–3.94 P=0.001) are risk factors for postoperative RFS. The impact of tumor max-diameter on RFS may be reflected in: First, larger tumors are typically associated with a higher probability of microvascular invasion and micrometastasis, which are key factors contributing to early postoperative recurrence and distant metastasis;27 second, larger tumors may represent a more aggressive tumor biological phenotype, leading to early postoperative recurrence.28 Prolonged PT reflects impaired hepatic synthetic function, particularly reduced synthesis of coagulation factors II, VII, IX, and X. This indicates more severe underlying liver disease, leading to poor postoperative recovery capacity and increased complication risk, thereby shortening RFS.29 These findings should be interpreted in the context that death prior to recurrence appeared to be rare in this cohort and therefore unlikely to materially affect the RFS analysis.
It is notable that the high ACCI group (scores> 4) represents a risk factor for both OS (Table 4) and RFS (Table 5). Possible reasons include: 1. Patients with high ACCI scores typically present with more severe and diverse comorbidities and older age. Consequently, their physiological reserves and capacity to cope with treatment (even minimally invasive RFA) are diminished. Comorbidities may also impact their tolerance and completion of subsequent necessary treatments (such as re-ablation after recurrence or TACE), thereby affecting long-term OS. 2. Patients with high ACCI scores face higher risks of non-tumor-related mortality (eg., cardiovascular events, multi-organ failure), which directly impacts OS. 3. Comorbidities like diabetes and cardiovascular disease may influence tumor recurrence and progression through mechanisms such as chronic inflammation and immunosuppression.30,31
In previous studies, ACCI has been used to predict postoperative outcomes following HCC resection13 and efficacy in RFA treatment for lung cancer,12 demonstrating good predictive performance with validated clinical value. However, its prognostic value in HCC patients undergoing RFA has been less extensively studied. This study provides incremental evidence for the predictive utility of ACCI in assessing outcomes of HCC patients with chronic comorbidities treated with RFA. This patient population often cannot undergo surgical resection due to a high burden of comorbidities, making RFA a safer treatment option.
For patients with chronic comorbidities who opt for the relatively safer RFA treatment, postoperative efficacy may vary due to differences in the types and severity of comorbidities among individuals. However, previous clinical practice lacked a quantitative indicator enabling clinicians to gain a relatively clear understanding of postoperative outcomes after RFA. ACCI may serve as a simple, low-cost, and readily available tool for preoperative risk stratification. Clinicians can rapidly calculate ACCI score preoperatively to identify high-risk patients, thereby strengthening perioperative comorbidities management (eg., consulting cardiology or endocrinology to optimize treatment plans). This ensures patients can tolerate the treatment and achieve favorable postoperative outcomes. Based on ACCI scores, clinicians may implement more active follow-up plans (eg., shortening follow-up intervals) to detect recurrence promptly after discharge, or conduct more careful benefit-risk assessments during multidisciplinary team discussions for high-risk patients. ACCI also facilitates more objective prognosis communication and expectation management with patients and their families.
This study has several limitations. First, it is a retrospective design, and data collection relies on the accuracy of medical records, which may introduce selection and information bias. Second, this is a single-center study with a relatively limited sample size, which may reduce statistical power, particularly for subgroup analyses. Additionally, the long follow-up time span and potential heterogeneity in treatment methods and perioperative management may influence the results. Given the relatively limited sample size and number of events, the use of stepwise variable selection may introduce a risk of overfitting and model instability. Although internal validation using bootstrap resampling demonstrated acceptable performance, the findings should still be interpreted with caution. Competing risks were not formally modeled and may influence the interpretation of overall survival. Future studies using competing risk models, such as the Fine–Gray subdistribution hazard model, are warranted to further clarify the impact of non-cancer mortality. Additionally, the cutoff determined by X-tile may be cohort-specific and requires external validation in independent populations. Continuous variables were dichotomized based on clinically established thresholds commonly used in clinical practice, which may lead to information loss and should be interpreted with caution. The study population primarily consists of HBV-related HCC, and the generalizability of these findings to populations with HCV- or non-viral hepatitis-dominant HCC remains to be established. Antiviral therapy was commonly administered in this cohort and therefore was not included as a covariate, which may introduce residual confounding. Prospective, multicenter studies with larger cohorts are warranted to further validate these findings and refine risk stratification models.
Conclusion
ACCI may serve as a useful prognostic predictor for survival outcomes of HCC patients with comorbidities undergoing RFA. It enables clinicians to preoperatively identify high-risk patients, thereby optimizing management strategies for comorbidities, developing individualized treatment and follow-up strategies, and facilitating more objective prognostic discussions with patients.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, [K.M], upon reasonable request.
Funding
This work was funded by the National Natural Science Foundation of China (No. 82073346).
Disclosure
Yuzheng Yan and Sijie Xiao are co-first authors of this research. The authors report there are no competing interests to declare.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. 2024;74(3):229–13. doi:10.3322/caac.21834
2. Vogel A, Chan SL, Dawson LA, et al. Hepatocellular carcinoma: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2025;36(5):491–506. doi:10.1016/j.annonc.2025.02.006
3. Singal AG, Llovet JM, Yarchoan M, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922–1965. doi:10.1097/HEP.0000000000000466
4. Zhou J, Sun H, Wang Z, et al. China liver cancer guidelines for the diagnosis and treatment of hepatocellular carcinoma (2024 edition). Liver Cancer;2025. 1–57. doi:10.1159/000546574
5. Association between multimorbidity and postoperative mortality in patients undergoing major surgery: a prospective study in 29 countries across Europe. Anaesthesia. 2024;79(9):945–956. doi:10.1111/anae.16324
6. Qu WF, Zhou PY, Liu WR, et al. Age-adjusted Charlson Comorbidity Index predicts survival in intrahepatic cholangiocarcinoma patients after curative resection. Ann translat Med. 2020;8(7):487. doi:10.21037/atm.2020.03.23
7. Suidan RS, Leitao MM Jr, Zivanovic O, et al. Predictive value of the Age-Adjusted Charlson Comorbidity Index on perioperative complications and survival in patients undergoing primary debulking surgery for advanced epithelial ovarian cancer. Gynecologic Oncol. 2015;138(2):246–251. doi:10.1016/j.ygyno.2015.05.034
8. Koppie TM, Serio AM, Vickers AJ, et al. Age-adjusted Charlson comorbidity score is associated with treatment decisions and clinical outcomes for patients undergoing radical cystectomy for bladder cancer. Cancer. 2008;112(11):2384–2392. doi:10.1002/cncr.23462
9. Park JW, Koh DH, Jang WS, et al. Age-adjusted Charlson Comorbidity Index as a prognostic factor for radical prostatectomy outcomes of very high-risk prostate cancer patients. PLoS One. 2018;13(6):e0199365. doi:10.1371/journal.pone.0199365
10. Asano T, Yamada S, Fujii T, et al. The Charlson age comorbidity index predicts prognosis in patients with resected pancreatic cancer. Int J Surg. 2017;39:169–175. doi:10.1016/j.ijsu.2017.01.115
11. Maezawa Y, Aoyama T, Kano K, et al. Impact of the Age-adjusted Charlson comorbidity index on the short- and long-term outcomes of patients undergoing curative gastrectomy for gastric cancer. J Cancer. 2019;10(22):5527–5535. doi:10.7150/jca.35465
12. Simon TG, Beland MD, Machan JT, Dipetrillo T, Dupuy DE. Charlson Comorbidity Index predicts patient outcome, in cases of inoperable non-small cell lung cancer treated with radiofrequency ablation. Eur. J. Radiol. 2012;81(12):4167–4172. doi:10.1016/j.ejrad.2012.06.007
13. Shinkawa H, Tanaka S, Takemura S, et al. Predictive value of the age-adjusted charlson comorbidity index for outcomes after hepatic resection of hepatocellular carcinoma. World J. Surg. 2020;44(11):3901–3914. doi:10.1007/s00268-020-05686-w
14. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
15. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–1251. doi:10.1016/0895-4356(94)90129-5
16. Dominguez DA, Wong P, Melstrom LG. Existing and emerging biomarkers in hepatocellular carcinoma: relevance in staging, determination of minimal residual disease, and monitoring treatment response: a narrative review. Hepatobiliary Surg. Nutr. 2024;13(1):39–55. doi:10.21037/hbsn-22-526
17. Liu G, Wang N, Zhang C, et al. Fructose-1,6-bisphosphate aldolase b depletion promotes hepatocellular carcinogenesis through activating insulin receptor signaling and lipogenesis. Hepatology. 2021;74(6):3037–3055. doi:10.1002/hep.32064
18. Huang Y, Xie Y, Zhang Y, et al. Single-cell transcriptome reveals the reprogramming of immune microenvironment during the transition from MASH to HCC. Mol Cancer. 2025;24(1):177. doi:10.1186/s12943-025-02370-2
19. Sun Y, Zhao M, Cheng L, et al. Reduction of alternative polarization of macrophages by short-term activated hepatic stellate cell-derived small extracellular vesicles. J Exp Clin Cancer Res. 2025;44(1):117. doi:10.1186/s13046-025-03380-0
20. Kitano S, Dolgor B. Does portal hypertension contribute to the pathogenesis of gastric ulcer associated with liver cirrhosis? J Gastroenterol. 2000;35(2):79–86. doi:10.1007/s005350050018
21. Voulgaris T, Karagiannakis D, Siakavellas S, et al. High prevalence of asymptomatic peptic ulcers diagnosed during screening endoscopy in patients with cirrhosis. Ann gastroenterol. 2019;32(5):451–456. doi:10.20524/aog.2019.0399
22. Pillai K, Akhter J, Chua TC, et al. Heat sink effect on tumor ablation characteristics as observed in monopolar radiofrequency, bipolar radiofrequency, and microwave, using ex vivo calf liver model. Medicine. 2015;94(9):e580. doi:10.1097/MD.0000000000000580
23. Bale R, Widmann G, Stoffner DI. Stereotaxy: breaking the limits of current radiofrequency ablation techniques. Eur. J. Radiol. 2010;75(1):32–36. doi:10.1016/j.ejrad.2010.04.013
24. Kim SK, Lim HK, Kim YH, et al. Hepatocellular carcinoma treated with radio-frequency ablation: spectrum of imaging findings. Radiographics. 2003;23(1):107–121. doi:10.1148/rg.231025055
25. Yang Y, Xin Y, Ye F, et al. Early recurrence after radiofrequency ablation for hepatocellular carcinoma: a multicenter retrospective study on definition, patterns and risk factors. Int J Hyperthermia. 2021;38(1):437–446. doi:10.1080/02656736.2020.1849828
26. Li JD, Xu XF, Han J, et al. Preoperative prealbumin level as an independent predictor of long-term prognosis after liver resection for hepatocellular carcinoma: a multi-institutional study. HPB. 2019;21(2):157–166. doi:10.1016/j.hpb.2018.06.1803
27. Rodríguez-Perálvarez M, Luong TV, Andreana L, Meyer T, Dhillon AP, Burroughs AK. A systematic review of microvascular invasion in hepatocellular carcinoma: diagnostic and prognostic variability. Ann Surg Oncol. 2013;20(1):325–339. doi:10.1245/s10434-012-2513-1
28. Hsu CC, Hsieh PM, Chen YS, et al. Axl and autophagy LC3 expression in tumors is strongly associated with clinical prognosis of hepatocellular carcinoma patients after curative resection. Cancer Med. 2019;8(7):3453–3463. doi:10.1002/cam4.2229
29. Wang XP, Mao MJ, He ZL, et al. A retrospective discussion of the prognostic value of combining prothrombin time(PT) and fibrinogen(Fbg) in patients with Hepatocellular carcinoma. J Cancer. 2017;8(11):2079–2087. doi:10.7150/jca.19181
30. Ogawa E, Kawano A, Kohjima M, et al. Long-term liver morbidity and mortality after hepatitis c virus elimination by direct-acting antivirals. J Gastroenterol Hepatol. 2025;40(4):971–978. doi:10.1111/jgh.16892
31. Koene RJ, Prizment AE, Blaes A, Konety SH. Shared risk factors in cardiovascular disease and cancer. Circulation. 2016;133(11):1104–1114. doi:10.1161/CIRCULATIONAHA.115.020406
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Delayed Hepatocellular Carcinoma Recurrence After Liver Transplantation: Comprehensive Clinical Characterization of Case Series
Wong TH, Ho CM, Hsu HH, Wu YM, Ho MC, Lee PH, Hu RH
Journal of Hepatocellular Carcinoma 2022, 9:1081-1091
Published Date: 17 October 2022
Thrombotic Thrombocytopenic Purpura After Radiofrequency Ablation of Hepatocellular Carcinoma: A Case Report
Chen R, Zhao Y, Umba Mabombo P, Hu H, Zhou X
Journal of Hepatocellular Carcinoma 2022, 9:1105-1108
Published Date: 26 October 2022
Prognostic Significance of Hemoglobin, Albumin, Lymphocyte and Platelet (HALP) Score in Hepatocellular Carcinoma
Zhou J, Yang D
Journal of Hepatocellular Carcinoma 2023, 10:821-831
Published Date: 2 June 2023
A Novel Four-Gene Signature Based on Nonsense-Mediated RNA Decay for Predicting Prognosis in Hepatocellular Carcinoma: Bioinformatics Analysis and Functional Validation
Zhao J, Wang C, Zhao L, Zhou H, Wu R, Zhang T, Ding J, Zhou J, Zheng H, Zhang L, Kong T, Zhou J, Hu Z
Journal of Hepatocellular Carcinoma 2024, 11:747-766
Published Date: 23 April 2024
Portal Venous and Hepatic Arterial Coefficients Predict Post-Hepatectomy Overall and Recurrence-Free Survival in Patients with Hepatocellular Carcinoma: A Retrospective Study
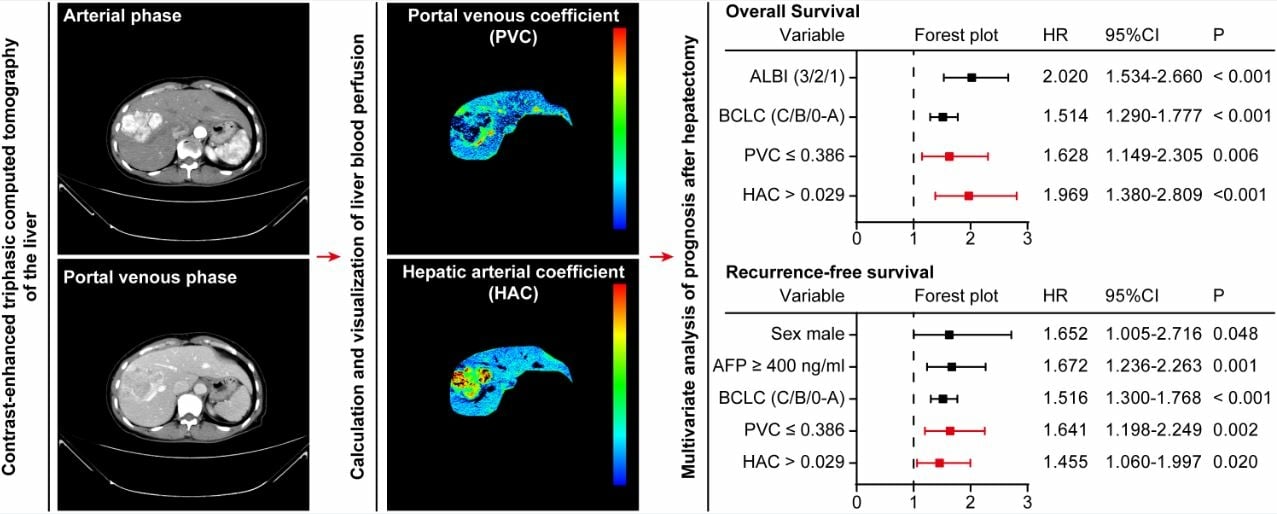
Li YK, Wu S, Wu YS, Zhang WH, Wang Y, Li YH, Kang Q, Huang SQ, Zheng K, Jiang GM, Wang QB, Liang YB, Li J, Lakang Y, Yang C, Li J, Wang JP, Kui X, Ke Y
Journal of Hepatocellular Carcinoma 2024, 11:1389-1402
Published Date: 9 July 2024