Back to Journals » International Journal of Women's Health » Volume 16

Predictors of Post-Caesarean Surgical Site Infections at Mubende Regional Referral Hospital, Central Uganda: Prospective Cohort Study (July–September 2023)
Authors Omara S ![]() , Kasujja M
, Kasujja M ![]() , Okot G, Okello P, Okello M, Mulumba R, Barageine JK
, Okot G, Okello P, Okello M, Mulumba R, Barageine JK
Received 22 August 2024
Accepted for publication 15 November 2024
Published 18 November 2024 Volume 2024:16 Pages 1939—1945
DOI https://doi.org/10.2147/IJWH.S482864
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Samuel Omara,1 Musa Kasujja,1 Geoffrey Okot,1 Peter Okello,1 Maxwell Okello,1 Richard Mulumba,1 Justus Kafunjo Barageine2
1Department of Obstetrics and Gynecology, Kampala International University Western Campus, Bushenyi, Uganda; 2Department of Obstetrics and Gynecology, Makerere University/Mulago Hospital, Kampala, Uganda
Correspondence: Samuel Omara, Email [email protected]
Background: Post-caesarean surgical site infections (PCSSIs) significantly impact maternal morbidity, mortality, and healthcare costs in low- and middle-income countries, particularly in sub-Saharan Africa, where preventive measures are often inadequate. Despite this burden, data on PCSSIs in this context are limited. This study aimed to evaluate the incidence and factors associated with PCSSIs at Mubende Regional Referral Hospital.
Methods: This prospective cohort study included 204 women who underwent caesarean sections from July to September 2023. Data was collected and participants were monitored for up to 28 days post-delivery to identify occurrences of surgical site infections (SSIs). Statistical analysis was conducted using STATA, with significance defined as a p-value of < 0.05.
Results: Most participants (63.2%) were aged 18– 35 years, with over 67% having a parity of ≤ 4. Preoperative antibiotics were administered to 77.5% of participants. Most surgeries (64.2%) lasted 1– 2 hours, and the overall incidence of surgical site infections (SSIs) was 16.18%. Significant risk factors associated with more than a twofold increase in SSI risk included unstable referral status (aRR = 2.02), obstructed labor (aRR = 2.97), chorioamnionitis (aRR = 2.73), and prolonged premature rupture of membranes (PROM) (aRR = 2.05). Prolonged labor increased SSI risk by 1.37-fold (aRR = 1.37), while receipt of preoperative antibiotics was linked to a reduced SSI risk (aRR = 0.77).
Conclusion: The post-caesarean SSI rate at Mubende Regional Referral Hospital is notably high, with key risk factors including unstable referral status, obstructed labor, prolonged labor, chorioamnionitis, and prolonged premature rupture of membranes (PROM). Administering preoperative antibiotics 30 minutes to 1 hour prior to surgery is linked to a reduced risk of SSI.
Keywords: caesarean section, surgical site infection, Uganda
Background
Post-caesarean surgical site infection (PCSSI) significantly contributes to maternal morbidity and mortality, resulting in extended hospital stays and increased healthcare costs.1–3 It adversely impacts women’s physical, emotional, reproductive, and psychosocial well-being.4
Globally, PCSSI rates are notably higher in low- and middle-income countries, especially in sub-Saharan Africa, compared to high-income countries (HICs), due to less effective preventive measures.4,5 Incidence rates in HICs such as the USA, Mainland China, South Korea, and the UK range from 0.5% to 4.5%,2,3,6 while in sub-Saharan Africa, rates range from 7% to 26%.1,3,7
Surgical site infections (SSIs) are classified as superficial, deep, or organ/space based on infection depth.8 Superficial SSIs involve skin, deep SSIs affect deeper tissues, and organ/space SSIs involve organs.9 SSIs increase morbidity, mortality, and healthcare costs. Prevention includes hand hygiene, preoperative antiseptic bathing, prophylactic antibiotics, and maintaining sterile conditions to mitigate infection risk.10
Risk factors for PCSSI vary by healthcare setting. Host-related factors include advanced maternal age, BMI > 30 kg/m², diabetes mellitus, hypertension, and multiple pregnancies. Antenatal issues such as limited visits, smoking, and alcohol use are also significant. Intrapartum factors like excessive vaginal examinations, chorioamnionitis, and prolonged operation duration further contribute.2,3 Additionally, anemia and postoperative hematoma are noted in some settings.2,11
Factors such as prolonged premature rupture of membranes, obstructed labor, extended operative time, and emergency operations increase wound contamination risk, even in hospitals with modern protocols.3,12 Other contributors include immunocompromised status, malnutrition, inadequate antibiotic selection, poverty, and environmental pollution, including the operating theatre environment.3,12
Given the variability in risk factors across healthcare facilities, even within the same locality, facility-specific identification is crucial. This approach allows for the development of targeted preventive measures and protocols by addressing host, microbial, and environmental factors to optimize patient outcomes.13,14
Despite the significant burden of PCSSI, detailed data at the individual hospital level in Uganda is limited due to budget constraints and competing resource priorities. Consequently, this study aimed to assess the incidence and risk factors associated with post-caesarean SSI at Mubende Regional Referral Hospital.
Materials and Methods
This prospective cohort study assessed 204 mothers who underwent caesarean sections at Mubende Regional Referral Hospital, Central Uganda, from July to September 2023. Surgical site infections (SSIs) were classified as superficial, deep, or organ/space.
Inclusion criteria encompassed all mothers who had a caesarean delivery during the study period, while those with pre-existing conditions such as diabetes or hypertension were excluded.
Sample size calculation. In a study conducted at Mulago National Referral Hospital in Uganda, the incidence of post caesarean surgical site infections was reported to be 7%.4 To determine the appropriate sample size for this study, the modified Daniel’s formula was utilized. The formula is as follows:
where: p=represents the incidence rate from similar studies, which is 7% (0.07), zα =is the standard normal variate at a significance level of 0.05, which is 1.96. zβ =is the standard normal variate at a power of 84%, which is 0.84. d=is the desired precision, set at 5% (0.05). By substituting these values into the formula, the required sample size is calculated as follows = 204.
Study Procedure
Eligible mothers who consented had their sociodemographic and obstetric data collected post-operatively from patient and operation files. They were monitored for SSI development for 28 days post-operatively, with follow-up through the obstetrics and gynecology outpatient clinics. Those who missed scheduled reviews were contacted by phone.
Data Analysis
The incidence of post-caesarean surgical site infection was analyzed descriptively and reported as a percentage. Demographic and obstetric characteristics were summarized using frequencies and percentages. Associations with post-caesarean surgical site infection were assessed with binomial regression and reported as relative risks. Variables with p ≤0.2 in bivariate analysis were included in multivariable analysis to control for confounders. Statistical significance was set at p ≤0.05.
Results
Among the 204 recruited mothers, 63.2% were between 18 and 35 years old. More than 67% had a parity of ≤4, and just 77.5% received preoperative antibiotics. Most surgeries (64.2%) lasted between 1 and 2 hours. Detailed patient characteristics are provided in Table 1.
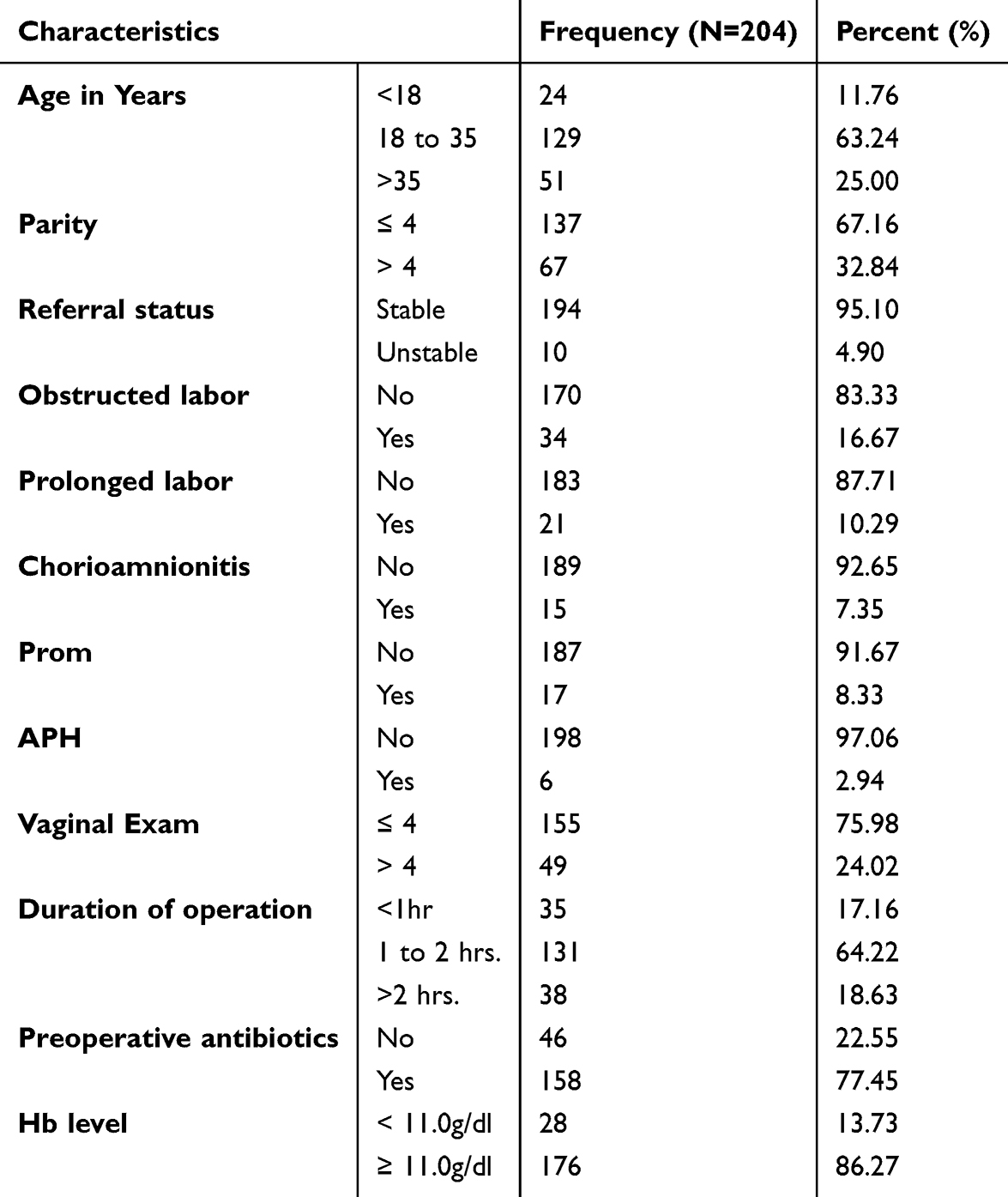 |
Table 1 Below Shows the Descriptive Statistics for Socio-Demographic, Obstetrical, and Interventional Characteristics of the Study Population |
The incidence of surgical site infection following caesarean sections was 16.18% (Table 2).
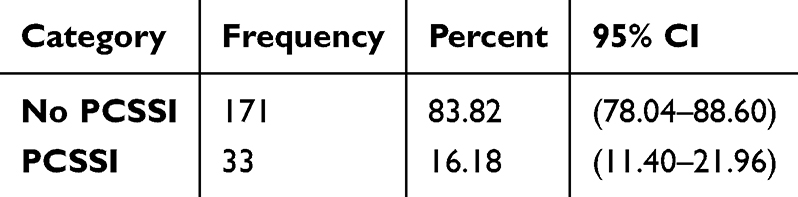 |
Table 2 Incidence of Post-Caesarean Surgical Site Infections Among Women Who Delivered by Caesarean Section at Mubende Regional Referral Hospital |
In the bivariate analysis, factors with a p-value of ≤0.2 were further examined in multivariate analysis to control for potential confounders. Receipt of pre-operative antibiotics correlated with a reduced risk of post-caesarean SSI (aRR = 0.77, CI: 0.77–0.77, p < 0.001).
Conversely, being referred as unstable, experiencing obstructed labor, chronic chorioamnionitis, and prolonged premature rupture of membranes (PROM) were each linked to more than a twofold increased risk of SSI (aRR = 2.02, CI: 1.58–2.57, p < 0.001; aRR = 2.97, CI: 1.84–4.79, p < 0.001; aRR = 2.73, CI: 1.90–3.91, p < 0.001; aRR = 2.05, CI: 1.27–3.30, p = 0.003, respectively). Prolonged labor was associated with a 1.37-fold increased risk of post-caesarean SSI (aRR = 1.37, CI: 1.07–1.74, p = 0.012) (see Table 3).
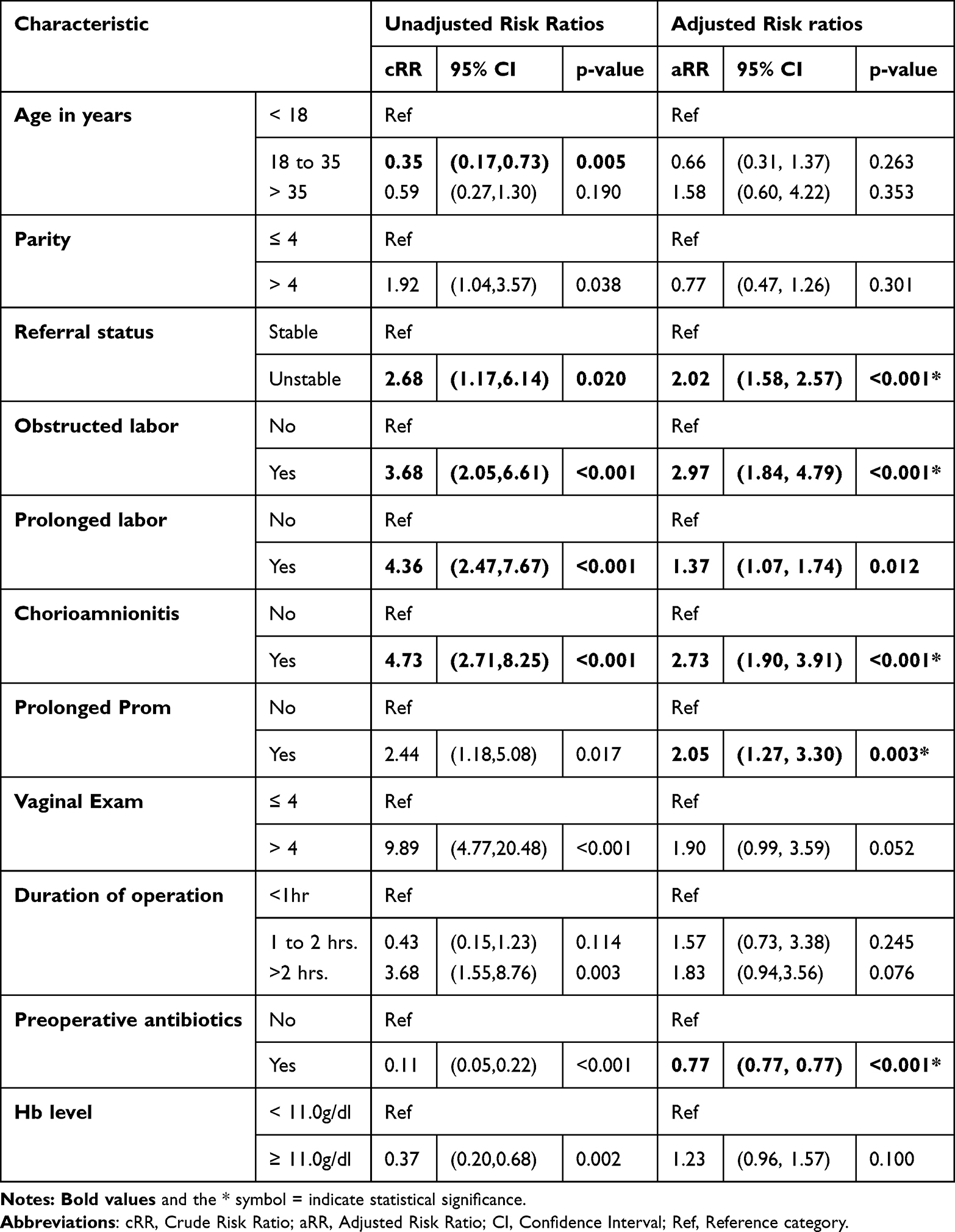 |
Table 3 Factors Associated with Post Caesarean Surgical Site Infection |
Discussion
Socio-Demographic, Obstetrical, and Interventional Characteristics
The study revealed that 63.2% of the population were young adults aged 18–35 years, with 67% of mothers who underwent caesarean delivery having four or fewer children. These findings align with Patamasingh et al,15 who reported high caesarean rates among younger women with low parity. This trend emphasizes the need for targeted interventions to address the increasing caesarean rates in young, low-parity populations.16 This highlight concerns about unnecessary caesarean sections, raising healthcare costs and surgical risks, necessitating targeted interventions and further research to address underlying drivers.
And yet 77.5% of mothers received preoperative antibiotics, indicating suboptimal adherence to prophylactic guidelines and it’s similar to a study done by Odah et al.17 Administering antibiotics 30–60 minutes before incision is recommended for optimal efficacy. Given that 64.2% of surgeries lasted 1–2 hours, timely prophylaxis is essential to reduce postoperative infections which still similar to a study done by Muliani et al.18 Inadequate adherence increases infection risk, leading to prolonged hospital stays, higher healthcare costs, and maternal complications. Improved compliance through enhanced training, stricter protocols, and targeted interventions is essential to minimize infection rates and improve surgical outcomes.
Incidence of Post-Caesarean Surgical Site Infection
The incidence of post-caesarean surgical site infection in our study was 16.18%, aligning with the reported range of 7.0% to 26.0% in sub-Saharan Africa.2,19,20
However, this incidence is notably higher than the 7% reported in studies at Mulago and Mbarara Referral Hospitals.3,4 The disparity may be due to differences in study populations, with the former hospitals serving more urban areas and providing better healthcare services than Mubende Hospital.
Additionally, the incidence in our study was markedly higher than the 1.4% reported in the UAE and 3% in Israel, likely due to their more advanced healthcare services and stricter intervention protocols.14,21
This highlights the necessity for enhanced healthcare infrastructure and adherence to infection control protocols in rural hospitals. Targeted interventions, such as improved staff training, increased access to antibiotics, and strict protocol enforcement, are essential for reducing surgical site infections and improving maternal health outcomes. Investment in rural healthcare is critical for safety.
Factors Associated with Post-Caesarean Surgical Site Infection
Unstable referrals had twice the risk of developing SSI compared to stable referrals. This is consistent with Gelaw et al’s cross-sectional study in Ethiopia, which attributed the increased risk to advanced preoperative disease states that hinder postoperative recovery and extend hospital stays, thereby increasing infection risk.2 Patients with unstable referrals require thorough preoperative assessments to reduce SSI risk. Optimizing care pathways and enhancing support can improve recovery and decrease infection rates.
Obstructed labor was associated with a relative risk of over 2.9 for post-caesarean surgical site infection compared to unobstructed labor. This heightened risk arises from tissue damage, increased contamination during the procedure, and complications during delivery, which expose the incision to bacteria from the skin and genital tract. These findings align with those of Isanga et al; and Kawakita et al11,22 Identifying patients at risk for obstructed labor facilitates timely interventions and enhanced monitoring. Improved surgical techniques and infection control measures can significantly reduce post-caesarean infection rates.
Prolonged labor was associated with a 1.37-fold increased risk of SSI post-caesarean section, consistent with findings from Nigeria and Nepal that reported higher SSI risk in post-caesarean cases with prolonged labor. This increased risk may be due to multiple vaginal interventions and meconium contamination.12,19 These findings highlight the necessity of timely interventions during labor to reduce surgical site infections. Effective management and monitoring strategies are essential for improving maternal healthcare outcomes.
Chorioamnionitis was significantly associated with a 2.7-fold increased risk of SSIs, due to bacterial contamination from infected amniotic fluid during surgery. This result aligns with findings from Kawakita et al and Njoku et al, who reported a similar association.19,22 These results emphasize the importance of managing chorioamnionitis to mitigate surgical site infection risk. Early identification and treatment can reduce bacterial contamination and surgical site infection (SSI) rates. Effective screening and treatment protocols for chorioamnionitis are essential for improving surgical outcomes and minimizing infection-related complications.
Prolonged premature rupture of membranes was associated with a twofold increased risk of SSI. Similar findings were reported by Njoku et al in Nigeria, and by Gelaw, Alemye, and Samuel et al in Ethiopia.2,8,19,23 This increased risk is likely due to bacterial colonization of the membranes and the subsequent ascent of infection to the surgical site. Vigilant monitoring and timely interventions are critical, along with stringent infection control measures during surgery. Developing targeted guidelines for these patients can improve surgical outcomes and enhance maternal and neonatal health.
Mothers who received prophylactic pre-operative antibiotics were 0.77 times less likely to develop SSI. Administering antibiotics 30 minutes to 1 hour before surgery similarly reduced the risk of post-caesarean SSI in studies by Alfouzan et al in Kuwait, Kawakita et al, and Wekesa et al in Uganda.4,22,24 These findings highlight the importance of adhering to evidence-based guidelines for prophylactic antibiotic use to reduce surgical site infection (SSI) rates. Standardized protocols and staff training are essential for minimizing SSI risk, thereby improving maternal and neonatal health and enhancing surgical outcomes in obstetric settings.
Conclusions
The post-caesarean SSI rate at Mubende Regional Referral Hospital remains high.
Key risk factors include unstable referral status, obstructed labor, prolonged labor, chorioamnionitis, and prolonged PROM.
Conversely, administration of preoperative antibiotics within 30 minute-1 hour preoperatively, was associated with a reduced risk of post-caesarean SSI.
Recommendations
We recommend healthcare provider and patient education, emphasizing early referral and timely surgical intervention to reduce SSI risks associated with obstructed labor, prolonged labor, and prolonged PROM.
We further recommend implementing retraining programs for healthcare providers on the use of preoperative antibiotics.
Data Sharing Statement
All materials are accessible to any scientist seeking non-commercial utilization, without breaching the confidentiality of participants from the corresponding authors on reasonable request.
Ethical Approval and Consent to Participate
This study was performed in accordance with the Declaration of Helsinki and all methods were performed in accordance with the relevant guidelines and regulations. Ethical approval was granted by the Bishop Stuart University Research and Ethics committee (BSU-REC-2023-101) and All participants provided informed consent. Informed consent for participants under 18 years was obtained from parents or legal guardians, following ethical guidelines.
Acknowledgments
We thank all the patients who agreed to participate and cooperated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no competing interests.
References
1. Samuel M. Community Care. 2020. Your responsibility.
2. Gelaw KA, Aweke AM, Astawesegn FH, Demissie BW, Zeleke LB. Surgical site infection and its associated factors following cesarean section: a cross sectional study from a public hospital in Ethiopia. Patient Saf Surg. 2017;11(1):1–7. doi:10.1186/s13037-017-0131-3
3. Ngonzi J, Bebell LM, Fajardo Y, et al. Incidence of postpartum infection, outcomes and associated risk factors at Mbarara regional referral hospital in Uganda. BMC Pregnancy Childbirth. 2018;18(1):1–11. doi:10.1186/s12884-018-1891-1
4. Wekesa YN, Namusoke F, Sekikubo M, Mango DW, Bwanga F. Ceftriaxone- and ceftazidime-resistant Klebsiella species, Escherichia coli, and methicillin-resistant Staphylococcus aureus dominate caesarean surgical site infections at Mulago Hospital, Kampala, Uganda. SAGE Open Med. 2020;8:1.
5. Mezemir R, Olayemi O, Dessie Y. Incidence, Bacterial Profile and Predictors of Surgical Site Infection After Cesarean Section in Ethiopia, A Prospective Cohort Study. Int J Womens Health. 2023;15:1547–1560. doi:10.2147/IJWH.S425632
6. Hope D, Ampaire L, Oyet C, Muwanguzi E, Twizerimana H, Apecu RO. Antimicrobial resistance in pathogenic aerobic bacteria causing surgical site infections in Mbarara regional referral hospital, Southwestern Uganda. Sci Rep. 2019;9(1):1–10. doi:10.1038/s41598-019-53712-2.
7. Legesse Laloto T, Hiko Gemeda D, Abdella SH. Incidence and predictors of surgical site infection in Ethiopia: prospective cohort. BMC Infect Dis. 2017;17(1):1–10. doi:10.1186/s12879-016-2167-x
8. Alemye T, Id LO, Id GF, Merid M, Id M. Post cesarean section surgical site infection and associated factors among women who delivered in public hospitals in Harar city, Eastern Ethiopia: a hospital-based analytic cross-sectional study. PLoS One. 2021;1–12. doi:10.1371/journal.pone.0253194
9. Jamtsho S, Wangdi TD, Wangdi P, Wangdi P. Incidence and factors associated with surgical site infections at the surgical ward, National Referral Hospital, Bhutan. Bhutan Health J. 2019;5(1):14–19.
10. Ganam S, Sher T, Assy R, et al. Assessing the impact of enhanced hygiene precautions during the COVID-19 pandemic on surgical site infection risk in abdominal surgeries. BMC Surg. 2024;24(1). doi:10.1186/s12893-024-02548-3
11. Isanga J, Emmanuel B, Musa K, et al. Women’s Health Care The Prevalence, Risk Factors, and Bacterial Profile of Cesarean Surgical Site Infections at a University Teaching Hospital in South Western Uganda Research Article. Int J Women’s Health Care Int J. 2020;5(1):2020.
12. Regmi A, Ojha N, Singh M, Ghimire A, Kharel N. Risk Factors Associated with Surgical Site Infection following Cesarean Section in Tertiary Care Hospital, Nepal. International Journal of Reproductive Medicine. 2022;2022. doi:10.1155/2022/4442453
13. Gyawali B, Ramakrishna K, Dhamoon AS. Sepsis: the evolution in definition, pathophysiology, and management. SAGE Open Med. 2019;7. doi:10.1177/2050312119835043
14. Alnajjar MS. Surgical site infections following caesarean sections at Emirati teaching hospital: incidence and implicated factors. Sci Rep. 2020;2020(0123456789):1–9. doi:10.1038/s41598-020-75582-9
15. Na Ayudhaya PO, Kittikraisak W, Phadungkiatwatana P, et al. Evaluation of cesarean delivery rates and factors associated with cesarean delivery among women enrolled in a pregnancy cohort study at two tertiary hospitals in Thailand. BMC Pregnancy Childbirth. 2024;24(1):1–13.
16. Handayani F, Muhida V, Ismayanty D. Description of Age and Parity with the Occurrence of Sectio Caesarea in Maternity Women in Cilegon City Regional Hospital for the Period July - December 2023. J Appl Heal Res Dev. 2024;6(1):25–31. doi:10.58228/jahrd.v6i1.49
17. Odah A, Alhusban H, Kaff AA, Alkhawaldeh F, Alwraikat S, Alshoufeen S. Proper Timing for Administration of Prophylactic Intravenous Antibiotics for Elective Surgical Procedures. SAS J Surg. 2023;9(04):309–314. doi:10.36347/sasjs.2023.v09i04.017
18. Muliani N, Herawati F, Yulia R, Wijono H. Quantity and quality profiles of antibiotics pre, on, and post surgery in a hospital setting. Int J Clin Pharm. 2021;43(5):1302–1310. doi:10.1007/s11096-021-01251-0
19. Njoku CO, Njoku AN. Microbiological pattern of surgical site infection following caesarean section at the University of Calabar Teaching Hospital. Open Access Maced J Med Sci. 2019;7(9):1430–1435. doi:10.3889/oamjms.2019.286
20. Gomaa K, Abdelraheim AR, Gelany SE, Khalifa EM, Yousef AM, Hassan H. Incidence, risk factors and management of post cesarean section surgical site infection (SSI) in a tertiary hospital in Egypt: a five year retrospective study. BMC Pregnancy Childbirth. 2021;3:1–9.
21. Zuarez-Easton S, Zafran N, Garmi G, Salim R. Postcesarean wound infection: prevalence, impact, prevention, and management challenges. Int J Womens Health. 2017;9:81–88. doi:10.2147/IJWH.S98876
22. Kawakita T, Landy HJ. Surgical site infections after cesarean delivery: epidemiology, prevention and treatment. Matern Heal Neonatol Perinatol. 2017;3(1):1–9.
23. Wodajo S, Belayneh M, Gebremedhin S. Magnitude and Factors Associated With Post-Cesarean Surgical Site Infection at Hawassa University Teaching and Referral Hospital, Southern Ethiopia: a Cross-sectional Study. Ethiop J Health Sci. 2017;27(3):283–290. doi:10.4314/ejhs.v27i3.10
24. Alfouzan W, Al Fadhli M, Abdo N, Alali W, Dhar R. Surgical site infection following cesarean section in a general hospital in Kuwait: trends and risk factors. Epidemiol Infect. 2019;147:e287. doi:10.1017/S0950268819001675
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.